

Rapamycin weekly maintenance dosing and the potential efficacy of combination sorafenib plus rapamycin but not atorvastatin or doxycycline in tuberous sclerosis preclinical models
- PMID: 19368729
- PMCID: PMC2670829
- DOI: 10.1186/1471-2210-9-8
Rapamycin weekly maintenance dosing and the potential efficacy of combination sorafenib plus rapamycin but not atorvastatin or doxycycline in tuberous sclerosis preclinical models
Abstract
Background: Tuberous sclerosis complex (TSC) is an autosomal dominant tumor suppressor syndrome, characterized by hamartomatous growths in the brain, skin, kidneys, lungs, and heart, which lead to significant morbidity. TSC is caused by mutations in the TSC1 or TSC2 genes, whose products, hamartin and tuberin, form a tumor suppressor complex that regulates the PI3K/Akt/mTOR pathway. Early clinical trials show that TSC-related kidney tumors (angiomyolipomas) regress when treated with the mammalian target of rapamycin (mTOR) inhibitor, rapamycin (also known as sirolimus). Although side effects are tolerable, responses are incomplete, and tumor regrowth is common when rapamycin is stopped. Strategies for future clinical trials may include the investigation of longer treatment duration and combination therapy of other effective drug classes.
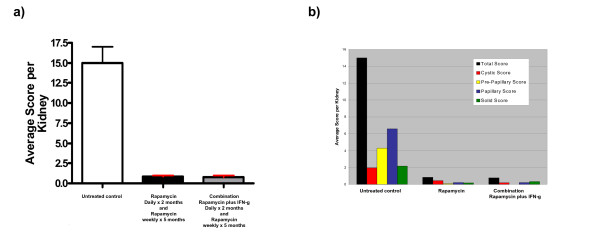
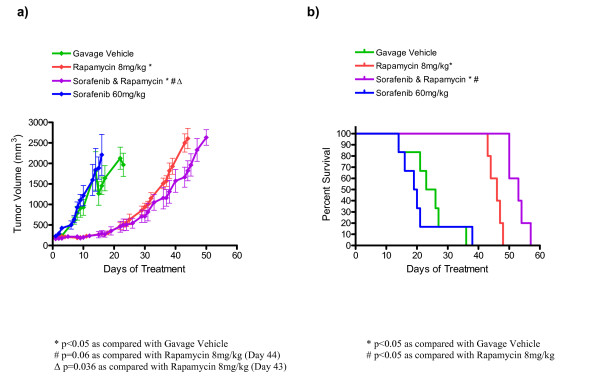
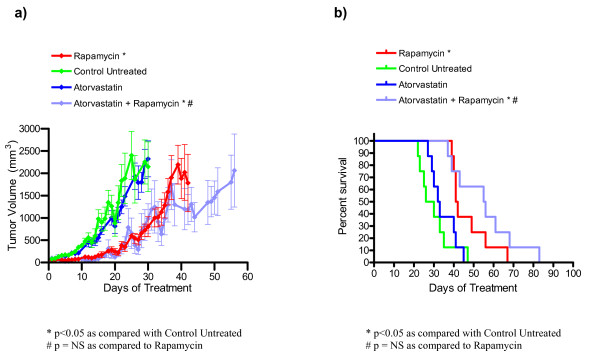
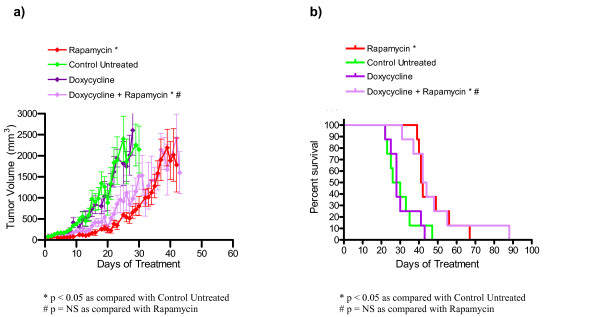
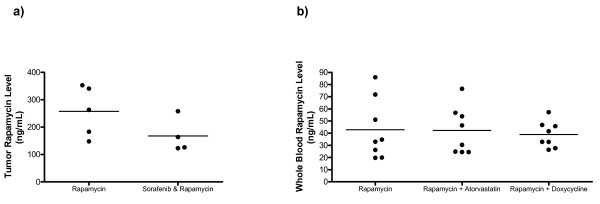
Results: Here, we examine the efficacy of a prolonged maintenance dose of rapamycin in Tsc2+/- mice with TSC-related kidney tumors. Cohorts were treated with rapamycin alone or in combination with interferon-gamma (IFN-g). The schedule of rapamycin included one month of daily doses before and after five months of weekly doses. We observed a 94.5% reduction in kidney tumor burden in Tsc2+/- mice treated (part one) daily with rapamycin (8 mg/kg) at 6 months <or= age < 7 months, (part 2) weekly with rapamycin (16 mg/kg) at 7 months <or= age < 12 months, and (part 3) daily with rapamycin (8 mg/kg) at 12 months <or= age < 13 months; but we did not observe any improvement with combination IFN-g plus rapamycin in this study. We also used a Tsc2-/- subcutaneous tumor model to evaluate other classes of drugs including sorafenib, atorvastatin, and doxycycline. These drugs were tested as single agents and in combination with rapamycin. Our results demonstrate that the combination of rapamycin and sorafenib increased survival and may decrease tumor volume as compared to rapamycin treatment alone while sorafenib as a single agent was no different than control. Atorvastatin and doxycycline, either as single agents or in combination with rapamycin, did not improve outcomes as compared with controls.
Conclusion: Our results indicate that prolonged treatment with low doses of mTOR inhibitors may result in more complete and durable TSC-related tumor responses, and it would be reasonable to evaluate this strategy in a clinical trial. Targeting the Raf/Mek/Erk and/or VEGF pathways in combination with inhibiting the mTOR pathway may be another useful strategy for the treatment of TSC-related tumors.
Figures
References
-
- Online Mendelian Inheritance in Man O . MIM number 191100. Baltimore, MD: Johns Hopkins University; 2003. http://www.ncbi.nlm.nih.gov/omim/
-
- Dabora SL, Jozwiak S, Franz DN, Roberts PS, Nieto A, Chung J, Choy YS, Reeve MP, Thiele E, Egelhoff JC, et al. Mutational Analysis in a Cohort of 224 Tuberous Sclerosis Patients Indicates Increased Severity of TSC2, Compared with TSC1, Disease in Multiple Organs. Am J Hum Genet. 2001;68:64–80. doi: 10.1086/316951. - DOI - PMC - PubMed
-
- Gomez M, Sampson J, Whittemore V, (eds.) The tuberous sclerosis complex. Third. Oxford, England: Oxford University Press; 1999.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
