

Impact of donor CMV status on viral infection and reconstitution of multifunction CMV-specific T cells in CMV-positive transplant recipients
- PMID: 19369230
- PMCID: PMC2710937
- DOI: 10.1182/blood-2009-02-203307
Impact of donor CMV status on viral infection and reconstitution of multifunction CMV-specific T cells in CMV-positive transplant recipients
Abstract
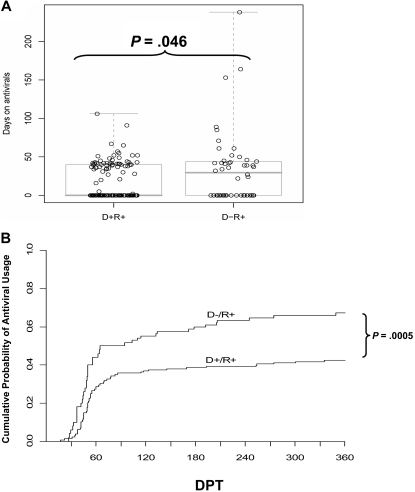
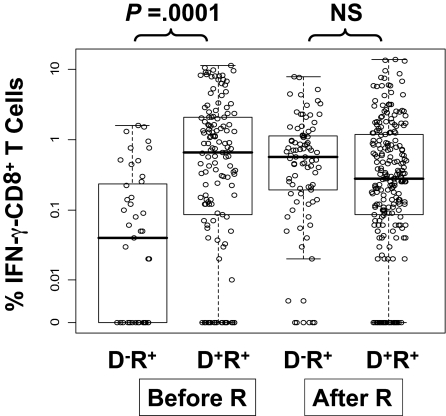
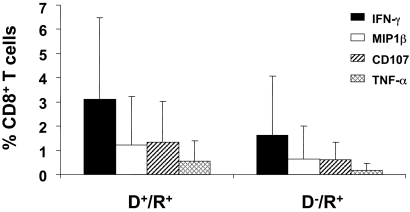
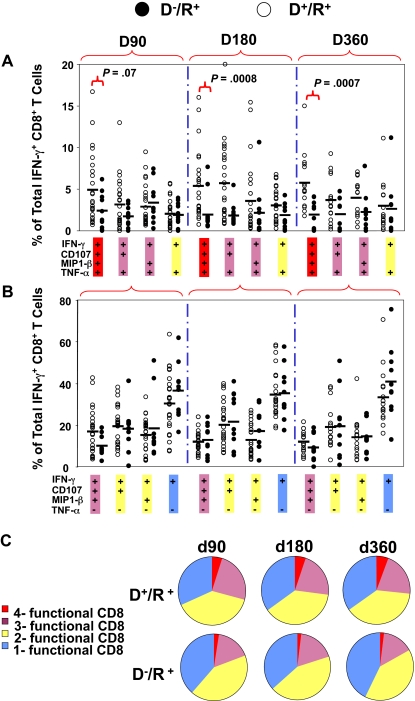
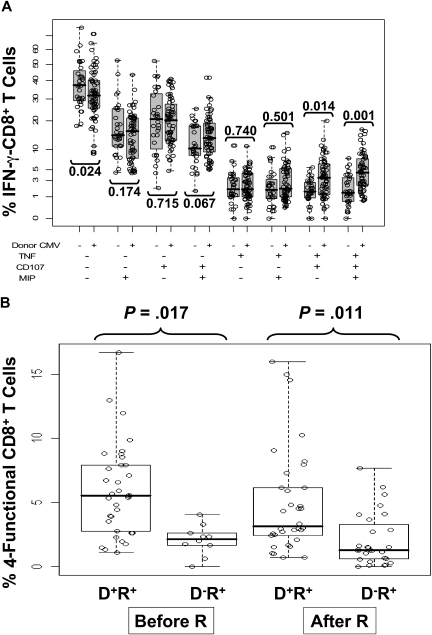
Reconstitution of cytomegalovirus (CMV)-specific CD8(+) T cells is essential to the control of CMV infection in CMV-positive recipients (R(+)) after allogeneic hematopoietic stem cell transplantation (HCT). Six-color flow cytometry was used to assess the functional profile of CMV-specific CD8(+) T cells in 62 of 178 R(+) HCT recipients followed virologically for CMV reactivation. R(+) recipients receiving grafts from CMV-negative donors (D(-); D(-)/R(+)) reconstituted fewer multifunctional CD8(+) T cells expressing tumor necrosis factor-alpha (TNF-alpha), macrophage inflammatory protein-1beta (MIP-1beta), and CD107 in addition to interferon-gamma (IFN-gamma), compared with D(+)/R(+) recipients. Unlike monofunctional CD8(+) T cells secreting IFN-gamma, which were abundantly generated during CMV reactivation in D(-)/R(+) recipients, the relative lack of multifunctional CD8(+) T cells persisted until at least 1 year post-HCT. D(-)/R(+) recipients were more likely to require recurrent and prolonged use of antivirals. These findings were robust to statistical adjustment for pretransplant factors, as well as for posttransplant factors including graft-versus-host disease (GVHD) and its treatment by steroids. These analyses suggest that D(+)/R(+) transplants, on average, generate higher levels of multifunctional CMV-specific T cells and require less antiviral therapy compared with D(-)/R(+) HCT recipients. These results highlight the benefit of D(+) donors in improving outcomes of R(+) HCT recipients by reducing the duration and recurrent need of antiviral treatment, aided by increased levels of multifunctional CMV-specific T cells.
Figures
References
-
- Nichols WG, Corey L, Gooley T, Davis C, Boeckh M. High risk of death due to bacterial and fungal infection among cytomegalovirus (CMV)-seronegative recipients of stem cell transplants from seropositive donors: evidence for indirect effects of primary CMV infection. J Infect Dis. 2002;185:273–282. - PubMed
-
- Schmidt GM, Horak DA, Niland JC, et al. A randomized, controlled trial of prophylactic ganciclovir for cytomegalovirus pulmonary infection in recipients of allogeneic bone marrow transplants; The City of Hope-Stanford-Syntex CMV Study Group. N Engl J Med. 1991;324:1005–1011. - PubMed
-
- Chakrabarti S, Mackinnon S, Chopra R, et al. High incidence of cytomegalovirus infection after nonmyeloablative stem cell transplantation: potential role of Campath-1H in delaying immune reconstitution. Blood. 2002;99:4357–4363. - PubMed
-
- Boeckh M, Nichols WG. The impact of cytomegalovirus serostatus of donor and recipient before hematopoietic stem cell transplantation in the era of antiviral prophylaxis and preemptive therapy. Blood. 2004;103:2003–2008. - PubMed
-
- Goodrich JM, Bowden RA, Fisher L, et al. Ganciclovir prophylaxis to prevent cytomegalovirus disease after allogeneic marrow transplant. Ann Intern Med. 1993;118:173–178. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- CA030206/CA/NCI NIH HHS/United States
- CA033572/CA/NCI NIH HHS/United States
- R01 CA077544/CA/NCI NIH HHS/United States
- R01 AI058148/AI/NIAID NIH HHS/United States
- AI058148/AI/NIAID NIH HHS/United States
- CA114889/CA/NCI NIH HHS/United States
- DK077374/DK/NIDDK NIH HHS/United States
- R21 AI062496/AI/NIAID NIH HHS/United States
- R21 DK077374/DK/NIDDK NIH HHS/United States
- P30 CA033572/CA/NCI NIH HHS/United States
- R01 CA145207/CA/NCI NIH HHS/United States
- P01 CA030206/CA/NCI NIH HHS/United States
- M01 RR000043/RR/NCRR NIH HHS/United States
- AI062496/AI/NIAID NIH HHS/United States
- M01-RR00043-39/RR/NCRR NIH HHS/United States
- CA077544/CA/NCI NIH HHS/United States
- R21 CA114889/CA/NCI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
