

Spondyloarthritis is associated with poor function and physical health-related quality of life
- PMID: 19369461
- PMCID: PMC2951477
- DOI: 10.3899/jrheum.081015
Spondyloarthritis is associated with poor function and physical health-related quality of life
Abstract
Objective: To study physical function and health-related quality of life (HRQOL) in US veterans with spondyloarthritis (SpA).
Methods: In a postal survey of 70,334 eligible veterans, demographics, performance of activities of daily living (ADL), and HRQOL, by Veterans Short Form-36, were queried; 58% responded (n = 40,508). Databases provided International Classification of Diseases, 9th ed. codes for ankylosing spondylitis (AS), psoriatic (PsA) and reactive arthritis (ReA), comorbidities, and demographics. Multivariable linear/logistic regressions compared ADL limitations and HRQOL in SpA versus non-SpA, and predictors in SpA.
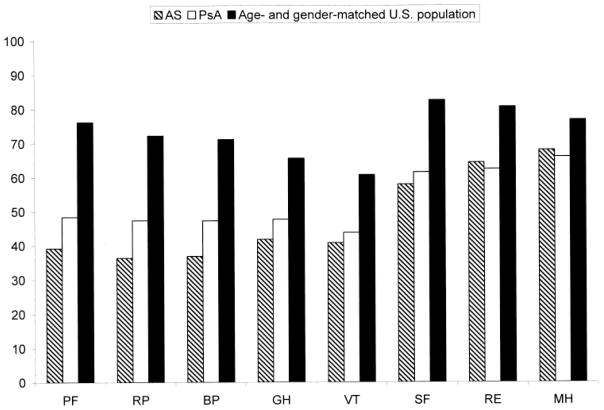
Results: Six hundred sixty-four veteran respondents had diagnoses of SpA: AS, n = 100; PsA, n = 551; ReA, n = 13. Veterans with AS, PsA, and ReA had significantly more limitations in dressing (44%, 23%, 24% vs 22%; p = 0.0002), transferring (57%, 42%, 64% vs 39%; p = 0.0006), walking (74%, 57%, 67% vs 54%; p = 0.0005), and overall mean ADL limitations (2.5, 1.7, 2.1 vs 1.6; p < 0.0001) compared to veterans without SpA, after multivariable adjustment. Limitations in each ADL in patients with SpA were 1.3-5.3 times that of an age-matched US cohort. Physical HRQOL was significantly lower compared with non-SpA veterans (p < 0.0001 for physical component summary, physical functioning, role physical, and bodily pain; p = 0.004 for general health) and age-sex-matched US norms; all differences exceeded clinically meaningful threshold of 5-10 units. More limitations in ADL were significantly associated with lower physical component summary scores in patients with AS and with lower physical and mental component summary scores in PsA.
Conclusion: After adjustment for differences in demographics and comorbidities, poorer physical function and HRQOL were observed in patients with SpA. Strategies focused to improve/maintain functional status are important for treatment of SpA.
Figures

References
-
- Salaffi F, De Angelis R, Stancati A, Grassi W. Health-related quality of life in multiple musculoskeletal conditions: A cross-sectional population based epidemiological study. II. The mapping study. Clin Exp Rheumatol. 2005;23:829–39. - PubMed
-
- Bostan EE, Borman P, Bodur H, Barca N. Functional disability and quality of life in patients with ankylosing spondylitis. Rheumatol Int. 2003;23:121–6. - PubMed
-
- Dagfinrud H, Kjeken I, Mowinckel P, Hagen KB, Kvien TK. Impact of functional impairment in ankylosing spondylitis: Impairment, activity limitation, and participation restrictions. J Rheumatol. 2005;32:516–23. - PubMed
-
- Doran MF, Brophy S, MacKay K, Taylor G, Calin A. Predictors of longterm outcome in ankylosing spondylitis. J Rheumatol. 2003;30:316–20. - PubMed
-
- Gran JT, Skomsvoll JF. The outcome of ankylosing spondylitis: A study of 100 patients. Br J Rheumatol. 1997;36:766–71. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous