

Calcifying pseudoneoplasms of the neuraxis: CT, MR imaging, and histologic features
- PMID: 19369614
- PMCID: PMC7051360
- DOI: 10.3174/ajnr.A1505
Calcifying pseudoneoplasms of the neuraxis: CT, MR imaging, and histologic features
Abstract
Background and purpose: Non-neoplastic, calcified, fibro-osseous lesions known as "calcifying pseudoneoplasms of the neuraxis" (CAPNON) are rare and can occur anywhere within the neuraxis. The radiologic and histopathologic characteristics of this unusual entity are not well understood. We present the largest series reviewing the MR imaging features of CAPNON.
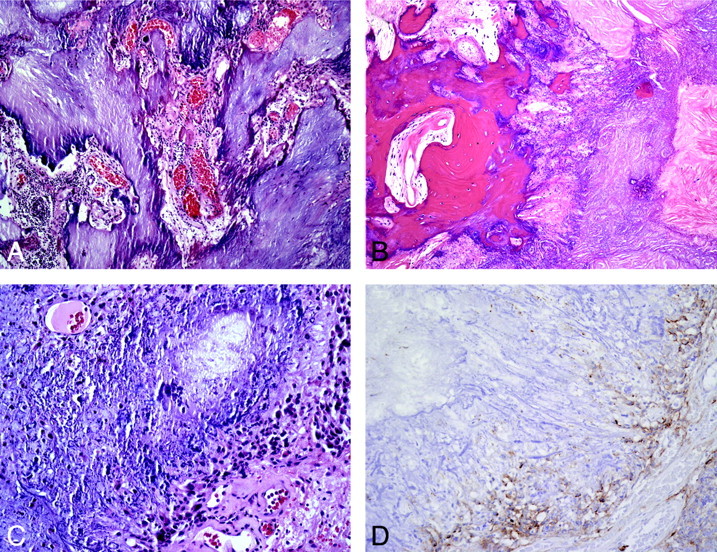
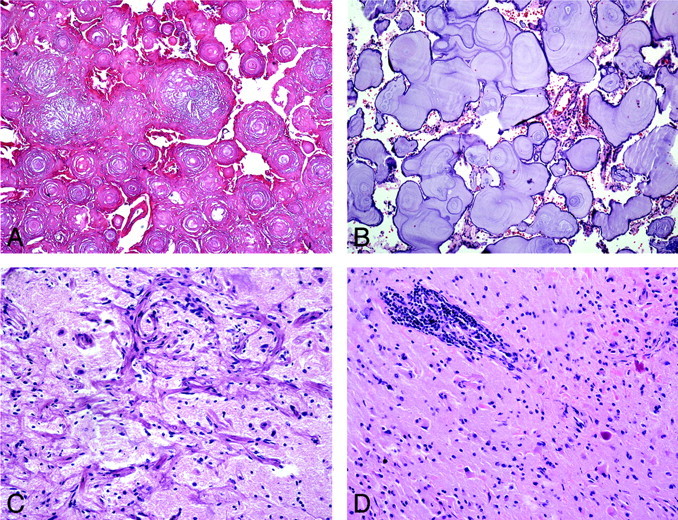
Materials and methods: The MR and CT imaging features in 4 patients with a pathologic diagnosis of "calcifying pseudoneoplasms of the neuraxis" were retrospectively reviewed. A neuropathologist also analyzed the histopathologic features for typical and atypical patterns.
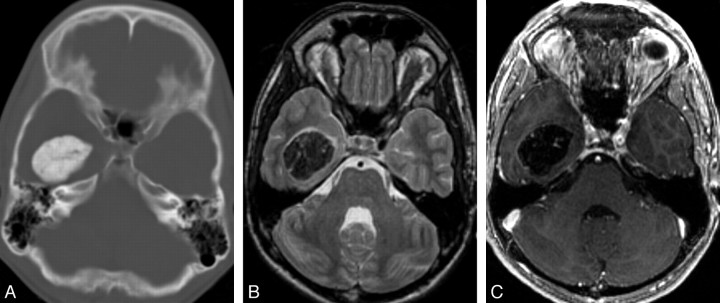
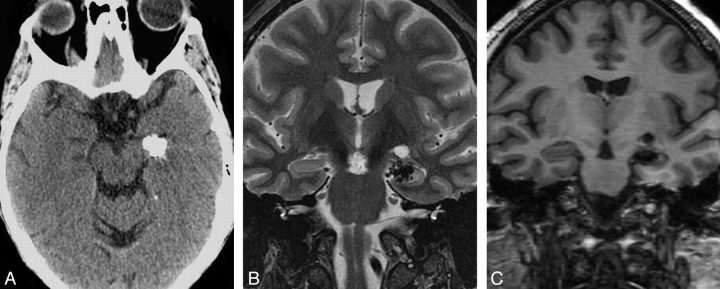
Results: Imaging features were strikingly similar for all 4 patients. All lesions appeared T1 and T2 hypointense without vasogenic edema. All tumors had dense calcification, and 3 tumors showed minimal linear internal or rim enhancement on MR imaging.
Conclusions: CAPNON may mimic more common vascular malformations or neoplasms and are often not considered in the differential diagnosis of calcified lesions. CAPNON should be included in the differential diagnosis of a calcified mass with marked T1 and T2 hypointensity and limited to no enhancement. Careful CT and MR imaging evaluation can suggest this entity, and this preoperative recognition may help subsequent management decisions.
Figures
Comment in
-
Choroid plexus papilloma with osseous metaplasia as a differential diagnosis of calcifying pseudoneoplasms of the neuraxis.AJNR Am J Neuroradiol. 2010 Jun;31(6):E51-2; author reply E53. doi: 10.3174/ajnr.A2096. Epub 2010 Apr 15. AJNR Am J Neuroradiol. 2010. PMID: 20395381 Free PMC article. No abstract available.
References
-
- Rhodes RH, Davis RL. An unusual fibro-osseous component in intracranial lesions. Hum Pathol 1978;9:309–19 - PubMed
-
- Bertoni F, Unni KK, Dahlin DC, et al. Calcifying pseudoneoplasms of the neural axis. J Neurosurg 1990;72:42–48 - PubMed
-
- Chang H, Park JB, Kim KW. Intraosseous calcifying pseudotumor of the axis: a case report. Spine 2000;25:1036–39 - PubMed
-
- Garen PD, Powers JM, King JS, et al. Intracranial fibro-osseous lesion. Case report. J Neurosurg 1989;70:475–77 - PubMed
-
- Jun C, Burdick B. An unusual fibro-osseous lesion of the brain. Case report. J Neurosurg 1984;60:1308–11 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical