

Male circumcision for prevention of heterosexual acquisition of HIV in men
- PMID: 19370585
- PMCID: PMC11666075
- DOI: 10.1002/14651858.CD003362.pub2
Male circumcision for prevention of heterosexual acquisition of HIV in men
Abstract
Background: Male circumcision is defined as the surgical removal of all or part of the foreskin of the penis and may be practiced as part of a religious ritual, as a medical procedure, or as part of a traditional ritual performed as an initiation into manhood. Since the 1980s, over 30 observational studies have suggested a protective effect of male circumcision on HIV acquisition in heterosexual men. In 2002, three randomised controlled trials to assess the efficacy of male circumcision for preventing HIV acquisition in men commenced in Africa. This review evaluates the results of these trials, which analysed the effectiveness and safety of male circumcision for preventing acquisition of HIV in heterosexual men.
Objectives: To assess the evidence of an interventional effect of male circumcision for preventing acquisition of HIV-1 and HIV-2 by men through heterosexual intercourse
Search strategy: We formulated a comprehensive and exhaustive search strategy in an attempt to identify all relevant studies regardless of language or publication status (published, unpublished, in press, and in progress). In June 2007 we searched the following electronic journal and trial databases: MEDLINE, EMBASE, and CENTRAL. We also searched the electronic conference databases NLM Gateway and AIDSearch and the trials registers ClinicalTrials.gov and Current Controlled Trials. We contacted researchers and relevant organizations and checked reference lists of all included studies.
Selection criteria: Randomised controlled trials of male circumcision versus no circumcision in HIV-negative heterosexual men with HIV incidence as the primary outcome.
Data collection and analysis: Two review authors independently assessed study eligibility, extracted data, and graded methodological quality. Data extraction and methodological quality were checked by a third author who resolved differences when these arose. Data were considered clinically homogeneous and meta-analyses and sensitivity analyses were performed.
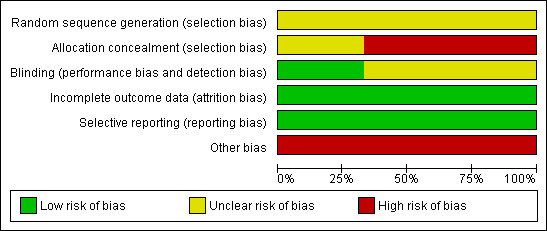
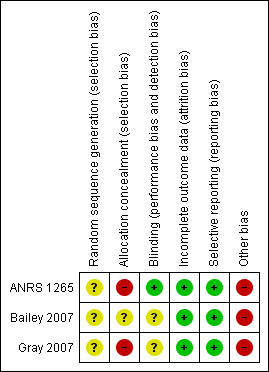
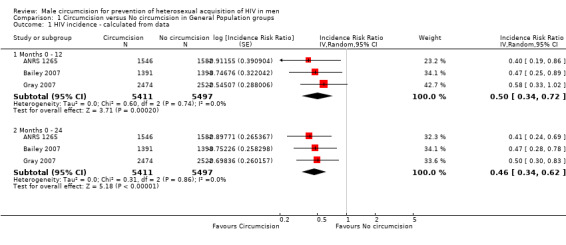
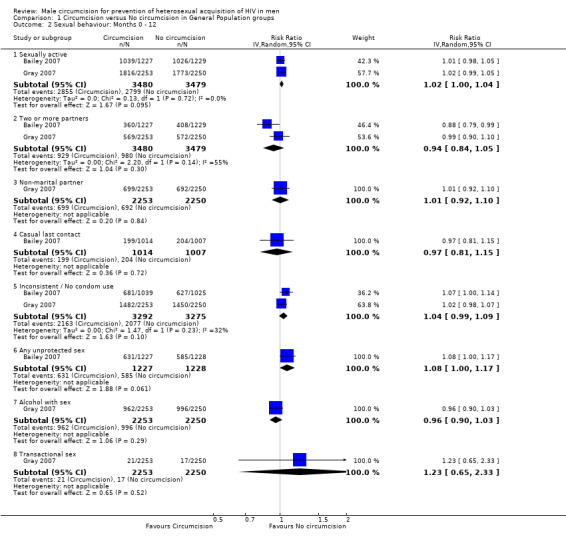
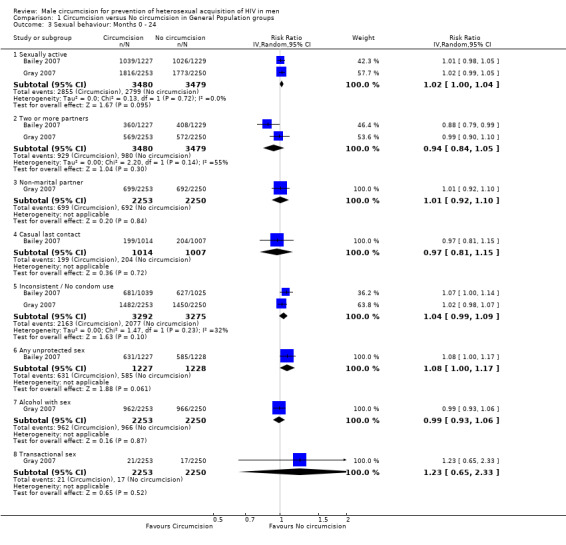
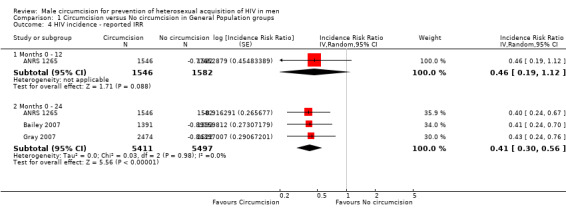
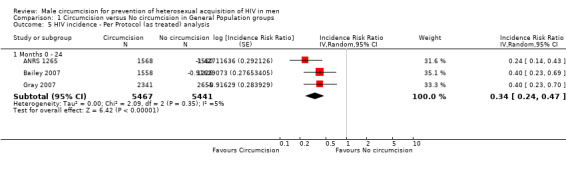
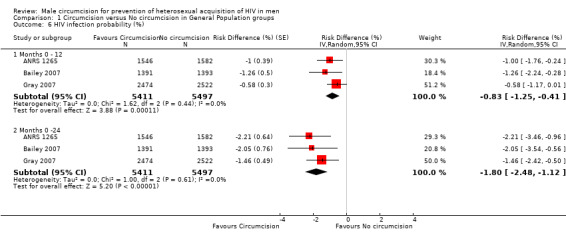
Main results: Three large RCTs of men from the general population were conducted in South Africa (N = 3 274), Uganda (N = 4 996) and Kenya (N = 2 784) between 2002 and 2006. All three trials were stopped early due to significant findings at interim analyses. We combined the survival estimates for all three trials at 12 months and also at 21 or 24 months in a meta-analysis using available case analyses using the random effects model. The resultant incidence risk ratio (IRR) was 0.50 at 12 months with a 95% confidence interval (CI) of 0.34 to 0.72; and 0.46 at 21 or 24 months (95% CI: 0.34 to 0.62). These IRRs can be interpreted as a relative risk reduction of acquiring HIV of 50% at 12 months and 54% at 21 or 24 months following circumcision. There was little statistical heterogeneity between the trial results (chi(2) = 0.60; df = 2; p = 0.74 and chi(2) = 0.31; df = 2; p = 0.86) with the degree of heterogeneity quantified by the I(2) at 0% in both analyses. We investigated the sensitivity of the calculated IRRs and conducted meta-analyses of the reported IRRs, the reported per protocol IRRs, and reported full intention-to-treat analysis. The results obtained did not differ markedly from the available case meta-analysis, with circumcision displaying significant protective effects across all analyses.We conducted a meta-analysis of the secondary outcomes measuring sexual behaviour for the Kenyan and Ugandan trials and found no significant differences between circumcised and uncircumcised men. For the South African trial the mean number of sexual contacts at the 12-month visit was 5.9 in the circumcision group versus 5 in the control group, which was a statistically significant difference (p < 0.001). This difference remained statistically significant at the 21-month visit (7.5 versus 6.4; p = 0.0015). No other significant differences were observed.Incidence of adverse events following the surgical circumcision procedure was low in all three trials.Reporting of methodological quality was variable across the three trials, but overall, the potential for significant biases affecting the trial results was judged to be low to moderate given the large sample sizes of the trials, the balance of possible confounding variables across randomised groups at baseline in all three trials, and the employment of acceptable statistical early stopping rules.
Authors' conclusions: There is strong evidence that medical male circumcision reduces the acquisition of HIV by heterosexual men by between 38% and 66% over 24 months. Incidence of adverse events is very low, indicating that male circumcision, when conducted under these conditions, is a safe procedure. Inclusion of male circumcision into current HIV prevention measures guidelines is warranted, with further research required to assess the feasibility, desirability, and cost-effectiveness of implementing the procedure within local contexts.
Conflict of interest statement
Nandi Siegfried, Martie Muller, Jimmy Volmink, and Jon Deeks were authors on the initial Cochrane review of observational studies (Siegfried 2003; Siegfried 2005). None have been involved in other previous research into the subject and are not currently involved in other related research.
Figures
Update of
-
Male circumcision for prevention of heterosexual acquisition of HIV in men.Cochrane Database Syst Rev. 2003;(3):CD003362. doi: 10.1002/14651858.CD003362. Cochrane Database Syst Rev. 2003. Update in: Cochrane Database Syst Rev. 2009 Apr 15;(2):CD003362. doi: 10.1002/14651858.CD003362.pub2. PMID: 12917962 Updated.
Comment in
-
Commentary: male circumcision for prevention of heterosexual acquisition of HIV in men: perspective from a trial team.Int J Epidemiol. 2010 Aug;39(4):970-1. doi: 10.1093/ije/dyq108. Epub 2010 Jul 12. Int J Epidemiol. 2010. PMID: 20624821 Free PMC article. No abstract available.
-
Commentary: one snip doesn't fit all.Int J Epidemiol. 2010 Aug;39(4):971-2. Int J Epidemiol. 2010. PMID: 20824909 No abstract available.
References
References to studies included in this review
ANRS 1265 {published data only}
Bailey 2007 {published data only}
-
- Bailey RC, Moses S, Parker CB, Agot K, Maclean I, Krieger JN, Williams CF, Campbell RT, Ndinya‐Achola JO. Male circumcision for HIV prevention in young men in Kisumu, Kenya: a randomised controlled trial. Lancet 2007;369(9562):643‐56. [1474‐547X (Electronic)] - PubMed
Gray 2007 {published data only}
-
- Gray RH, Kigozi G, Serwadda D, Makumbi F, Watya S, Nalugoda F, Kiwanuka N, Moulton LH, Chaudhary MA, Chen MZ, Sewankambo NK, Wabwire‐Mangen F, Bacon MC, Williams CF, Opendi P, Reynolds SJ, Laeyendecker O, Quinn TC, Wawer MJ. Male circumcision for HIV prevention in men in Rakai, Uganda: a randomised trial. Lancet 2007;369(9562):657‐66. [1474‐547X (Electronic)] - PubMed
Additional references
Bailey 2001
-
- Bailey RC, Plummer FA, Moses S. Male circumcision and HIV prevention: current knowledge and future research directions. The Lancet Infectious Diseases 2001;1:223‐30. - PubMed
Bailey 2008
Cold 1999
-
- Cold CJ, Taylor JR. The prepuce. British Journal of Urology 1999;83:34‐44. - PubMed
De Vincenzi 1994
-
- Vincenzi ID, Mertens T. Male circumcision: a role in HIV prevention?. AIDS 1994;8:153‐60. - PubMed
Donoval 2006
-
- Donoval BA, Landay AL, Moses S, Agot K, Ndinya‐Achola JO, Nyagaya EA, et al. HIV‐1 target cells in foreskins of African men with varying histories of sexually transmitted infections. Am J Clin Pathol 2006;125(3):386‐91. - PubMed
Fleiss 1998
Higgins 2002
-
- Higgins JP, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;21(11):1539‐58. - PubMed
Higgins 2008
-
- Higgens JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.0 [updated February 2008]. The Cochrane Collaboration, 2008. [Available from www.cochrane‐handbook.org]
Horizons 2000
-
- Horizons. Report: Male circumcision and HIV prevention: Directions for future research. Washington DC: Office of Health and Nutrition, Global Bureau, U.S. Agency for International Development 2000.
Hussain 1995
Kim 1987
-
- Kim K, DeMets DL. Design and analysis of group sequential tests based on the type 1 error spending rate function. Biometrika 1987;74:149‐54.
Lee‐Huang 1999
Mills 2006
-
- Mills E, Siegfried N. Cautious optimism for new HIV/AIDS prevention strategies. The Lancet 2006;368:1236. - PubMed
Montori 2005
-
- Montori VM, Devereaux PJ, Adhikari NK, et al. Randomized trials stopped early for benefit: a systematic review. JAMA 2005;294:2203‐09.. - PubMed
Moses 1994
-
- Moses S, Plummer FA, Bradley JE, Ndiya‐Achola JO, Nagelkerke NJD, Ronald AR. [The association between lack of male circumcision and risk for HIV infection: a review of the epidemiological data]. Sexually Transmitted Diseases 1994;21:201‐10. - PubMed
Moses 1998
Patterson 2002
-
- Patterson. American Journal of Pathology 2002;161.
Peltzer 2008
Soto‐Ramirez 1996
-
- Soto‐Ramirez LE, Renjifo B, McLane MF, Marlink R, O'Hara C, Sutthent R, Wasi C, Vithayasi P, Vithayasai V, Apichartpiyakul C, Auewarakul P, Cruz VP, Chui D‐S, Osathanondh R, Mayer K, Lee T‐H, Essex M. HIV‐1 Langerhans' cell tropism with heterosexual transmission of HIV. Science 1996;271:1291‐3. - PubMed
Szabo 2000
UNAIDS and WHO 2007
-
- UNAIDS, WHO. New data on male circumcision and HIVprevention: policy and programme implications; WHO/UNAIDStechnical consultation male circumcision and HIV prevention:research implications for policy and programming. Montreux, Geneva: Joint United Nations Programme on HIV/AIDS and WorldHealth Organization 2007.
Van Howe 1999
-
- Howe RS. Circumcision and HIV infection: review of the literature and meta‐analysis. International Journal of STD and AIDS 1999;10:8‐16. - PubMed
Wawer 2008
-
- Wawer M, Kigozi G, Serwadda D, Makumbi F, Nalugoda F, Watya S, Buwembo D, Ssempijja V, Moulton L, Gray R. Trial of circumcision in HIV+ men in Rakai, Uganda: effects in HIV+ men and women partners. Fifteenth Conference on Retroviruses and Opportunistic Infections. Boston, 2008; Vol. Abstract 33LB.
Weiss 2000
-
- Weiss HA, Quigley MA, Hayes R. Male circumcision and risk of HIV infection in sub‐Saharan Africa: a systematic review and meta‐analysis. AIDS 2000;14:2361‐70. - PubMed
References to other published versions of this review
Siegfried 2003
-
- Siegfried N, Muller M, Volmink J, Deeks J, Egger M, Low N, et al. Male circumcision for prevention of heterosexual acquisition of HIV in men. Cochrane Database Syst Rev 2003, (3):CD003362. - PubMed
Siegfried 2005
-
- Siegfried N, Muller M, Deeks J, Volmink J, Egger M, Low N, et al. HIV and male circumcision‐‐a systematic review with assessment of the quality of studies. Lancet Infect Dis 2005;5(3):165‐73. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous