

Intravenous or intramuscular parecoxib for acute postoperative pain in adults
- PMID: 19370610
- PMCID: PMC6540719
- DOI: 10.1002/14651858.CD004771.pub4
Intravenous or intramuscular parecoxib for acute postoperative pain in adults
Abstract
Background: Parecoxib was the first COX-2 available for parenteral administration, and may, given intravenously or intramuscularly, offer advantages over oral medication when patients have nausea and vomiting or are unable to swallow, such as in the immediate postoperative period.
Objectives: Assess the efficacy of single dose intravenous or intramuscular parecoxib in acute postoperative pain, the requirement for rescue medication, and any associated adverse events.
Search strategy: We searched Cochrane CENTRAL, MEDLINE, EMBASE in November 2008.
Selection criteria: Randomised, double-blind, placebo-controlled clinical trials of parecoxib compared with placebo for relief of acute postoperative pain in adults.
Data collection and analysis: Two review authors independently assessed trial quality and extracted data. The area under the "pain relief versus time" curve was used to derive the proportion of participants with parecoxib and placebo experiencing at least 50% pain relief over 6 hours, using validated equations. The number-needed-to-treat-to-benefit (NNT) was calculated using 95% confidence intervals (CI). The proportion of participants using rescue analgesia over a specified time period, and time to use of rescue analgesia, were sought as additional measures of efficacy. Information on adverse events and withdrawals were also collected.
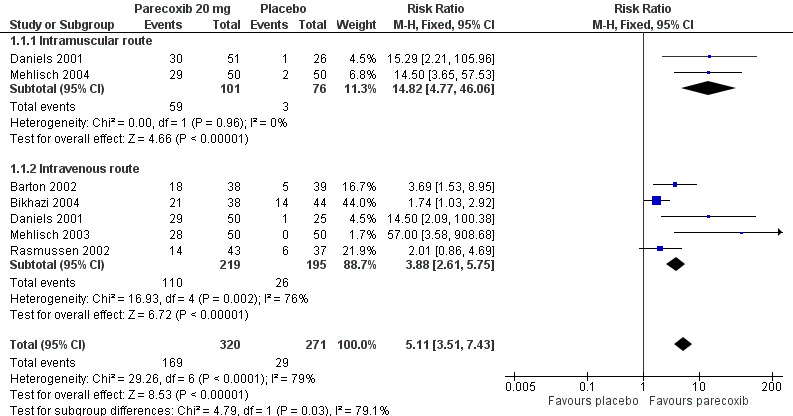
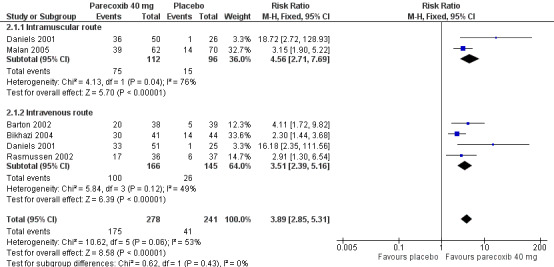
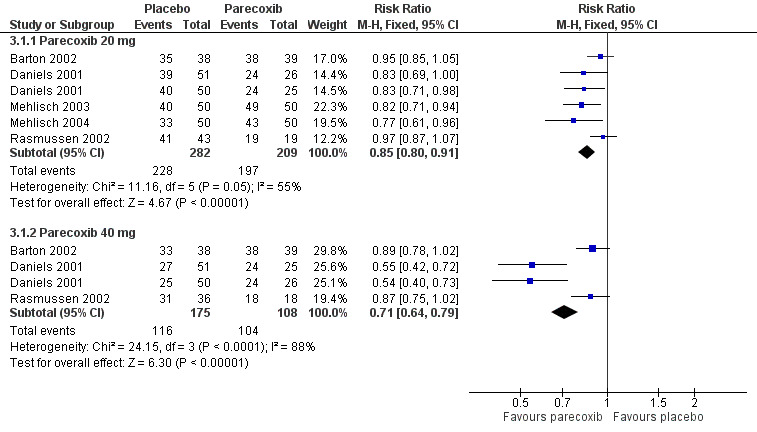
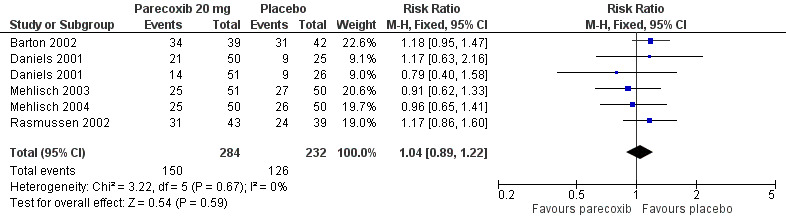
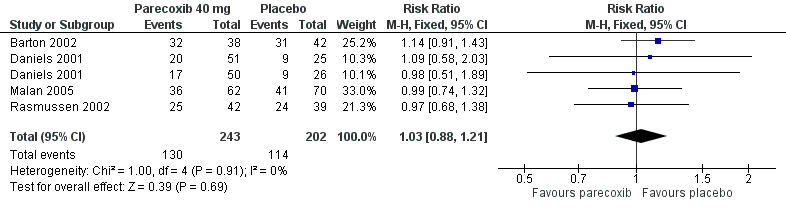
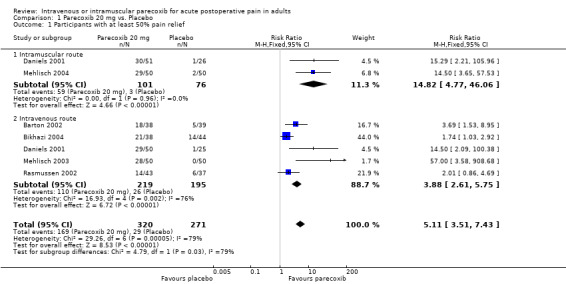
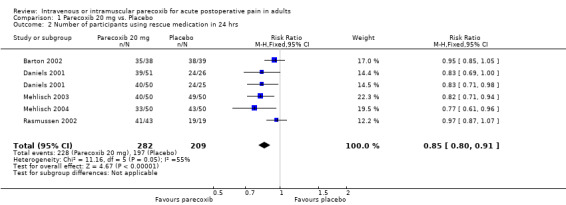
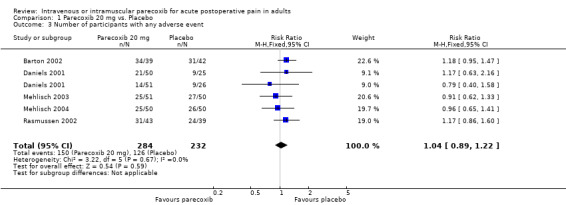
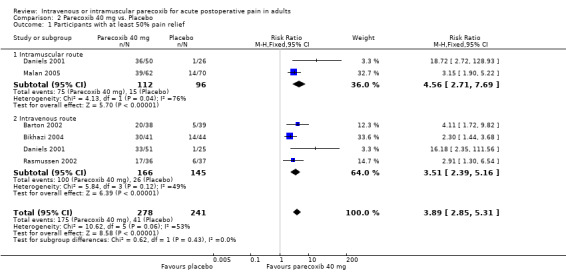
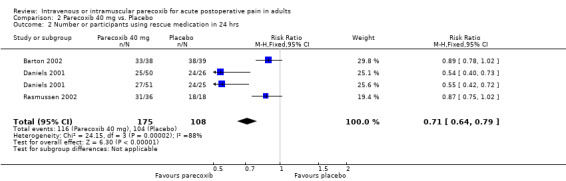
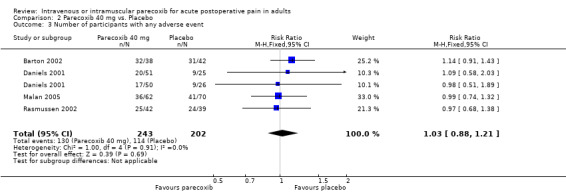
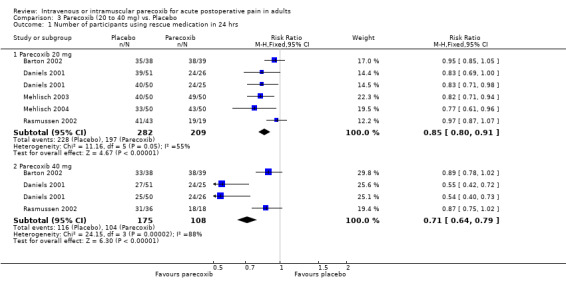
Main results: Seven studies (1446 participants) were included. There was no significant difference between doses, or between intravenous and intramuscular administration for 50% pain relief over 6 hours: NNTs compared with placebo were 3.1 (2.4 to 4.5), 2.4 (2.1 to 2.8), and 1.8 (1.5 to 2.3) for 10, 20, and 40 mg parecoxib respectively. Fewer participants required rescue medication over 24 hours with parecoxib than placebo: parecoxib 40 mg was significantly better than parecoxib 20 mg (NNTs to prevent use of rescue medication 7.5 (5.3 to 12.8) and 3.3 (2.6 to 4.5) respectively; P < 0.0007). Median time to use of rescue medication was 3.1 hours, 6.9 hours and 10.6 hours with parecoxib 10 mg, 20 mg and 40 mg respectively, and 1.5 hours with placebo. Adverse events were generally mild to moderate, rarely led to withdrawal, and did not differ in frequency between groups. No serious adverse events were reported with parecoxib or placebo.
Authors' conclusions: A single dose of parecoxib 20 mg or 40 mg provided effective analgesia for 50 to 60% of those treated compared to about 15% with placebo, and was well tolerated. Duration of analgesia was longer, and significantly fewer participants required rescue medication over 24 hours with the higher dose.
Conflict of interest statement
RAM, HJM and SD have received research support from charities, government and industry sources at various times, but no such support was received for this work. RAM and HJM have consulted for various pharmaceutical companies. RAM, and HJM have received lecture fees from pharmaceutical companies related to analgesics and other healthcare interventions.
Figures
Update of
- doi: 10.1002/14651858.CD004771.pub3
References
References to studies included in this review
Barton 2002 {published data only}
-
- Barton SF, Langeland FF, Snabes MC, LeComte D, Kuss ME, Dhadda SS, et al. Efficacy and safety of intravenous parecoxib sodium in relieving acute postoperative pain following gynecologic laparotomy surgery. Anesthesiology 2002;97(2):306‐14. - PubMed
Bikhazi 2004 {published data only}
-
- Bikhazi GB, Snabes MC, Bajwa ZH, Davis DJ, LeComte D, Traylor L, et al. A clinical trial demonstrates the analgesic activity of intravenous parecoxib sodium compared with ketorolac or morphine after gynecologic surgery with laparotomy. American Journal of Obstetrics and Gynecology 2004;191(4):1183‐91. [DOI: 10.1016/j.ajog.2004.05.006] - DOI - PubMed
Daniels 2001 {published data only}
-
- Daniels SE, Grossman EH, Kuss ME, Talwalker S, Hubbard RC. A double‐blind, randomized comparison of intramuscularly and intravenously administered parecoxib sodium versus ketorolac and placebo in a post‐oral surgery pain model. Clinical Therapeutics 2001;23(7):1018‐31. [DOI: 10.1016/S0149-2918(01)80088-6] - DOI - PubMed
Malan 2005 {published data only}
-
- Malan TP Jr, Gordon S, Hubbard R, Snabes M. The cyclooxygenase‐2‐specific inhibitor parecoxib sodium is as effective as 12 mg of morphine administered intramuscularly for treating pain after gynecologic laparotomy surgery. Anesthesia and Analgesia 2005;100(2):454‐60. [DOI: 10.1213/01.ANE.0000143355.52418.CF] - DOI - PubMed
Mehlisch 2003 {published data only}
Mehlisch 2004 {published data only}
-
- Mehlisch DR, Desjardins PJ, Daniels S, Hubbard RC. The analgesic efficacy of intramuscular parecoxib sodium in postoperative dental pain. The Journal of the American Dental Association 2004;135(11):1578‐90. - PubMed
Rasmussen 2002 {published data only}
-
- Rasmussen GL, Steckner K, Hogue C, Torri S, Hubbard RC. Intravenous parecoxib sodium for acute pain after orthopedic knee surgery. The American Journal of Orthopedics 2002;31(6):336‐43. - PubMed
References to studies excluded from this review
Hubbard 2003 {published data only}
-
- Hubbard RC, Naumann TM, Traylor L, Dhadda S. Parecoxib sodium has opioid‐sparing effects in patients undergoing total knee arthroplasty under spinal anaesthesia. British Journal of Anaesthesia 2003;90(2):166‐72. - PubMed
Jirarattanaphochai 2008 {published data only}
-
- Jirarattanaphochai K, Thienthong S, Sriraj W, Jung S, Pulnitiporn A, Lertsinudom S, et al. Effect of parecoxib on postoperative pain after lumbar spine surgery: a bicenter, randomized, double‐blinded, placebo‐controlled trial. Spine 2008;33(2):132‐9. - PubMed
Nussimeier 2006 {published data only}
-
- Nussmeier NA, Whelton AA, Brown MT, Joshi GP, Langford RM, Singla NK, et al. Safety and efficacy of the cyclooxygenase‐2 inhibitors parecoxib and valdecoxib after noncardiac surgery. Anesthesiology 2006;104(3):518‐26. - PubMed
Puolakka 2006 {published data only}
-
- Puolakka PA, Puura AI, Pirhonen RA, Ranta AU, Autio V, et al. Lack of analgesic effect of parecoxib following laparoscopic cholecystectomy. Acta Anaesthesiologica Scandinavica 2006;50(8):1027‐32. - PubMed
Snabes 2007 {published data only}
-
- Snabes MC, Jakimiuk AJ, Kotarski J, Katz TK, Brown MT, Verburg KM. Parecoxib sodium administered over several days reduces pain after gynecologic surgery via laparotomy. Journal of Clinical Anesthesia 2007;19(6):448‐55. - PubMed
Tang 2002 {published data only}
-
- Tang J, Li S, White PF, Chen X, Wender RH, Quon R, et al. Effect of parecoxib, a novel intravenous cyclooxygenase type‐2 inhibitor, on the postoperative opioid requirement and quality of pain control. Anesthesiology 2002;96(6):1305‐9. - PubMed
Viscusi 2008 {published data only}
-
- Viscusi ER, Gimbel JS, Halder AM, Snabes M, Brown MT, Verburg KM. A multiple‐day regimen of parecoxib sodium 20 mg twice daily provides pain relief after total hip arthroplasty. Anesthesia and Analgesia 2008;107(2):652‐60. - PubMed
References to studies awaiting assessment
Apfelbaum 2008 {published data only}
-
- Apfelbaum JL, Desjardins PJ, Brown MT, Verburg KM. Multiple‐day efficacy of parecoxib sodium treatment in postoperative bunionectomy pain. The Clinical Journal of Pain 2008;24(9):784‐92. - PubMed
Additional references
Barden 2002
Barden 2004
-
- Barden J, Edwards JE, McQuay HJ, Moore RA. Pain and analgesic response after third molar extraction and other postsurgical pain. Pain 2004;107(1‐2):86‐90. - PubMed
Barden 2005
Barden 2008
Clarke 2009
Collins 1997
-
- Collins SL, Moore RA, McQuay HJ. The visual analogue pain intensity scale: what is moderate pain in millimetres?. Pain 1997;72:95‐7. - PubMed
Collins 1999
Collins 2001
-
- Collins SL, Edwards J, Moore RA, Smith LA, McQuay HJ. Seeking a simple measure of analgesia for mega‐trials: is a single global assessment good enough?. Pain 2001;91:189‐94. - PubMed
Cook 1995
Cooper 1991
-
- Cooper SA. Single‐dose analgesic studies: the upside and downside of assay sensitivity. In: Max MB, Portenoy RK, Laska EM editor(s). The Design of Analgesic ClinicalTrials. Advances in Pain Research and Therapy. Vol. 18, New York: Raven Press, 1991:117‐24.
Derry 2008
Derry 2009a
Derry 2009b
Edwards 1999
-
- Edwards JE, McQuay HJ, Moore RA, Collins SL. Reporting of adverse effects in clinical trials should be improved: lessons from acute postoperative pain. Journal of Pain and Symptom Management 1999;18(6):427‐37. - PubMed
EMEA 2002
-
- The European Agency for the Evaluation of Medicinal Products. EMEA public statement on parecoxib sodium (Dynastat/Rayzon/Xapit): risk of serious hypersensitivity and skin reactions. EMEA (25175/02), 2002.
FitzGerald 2001
-
- FitzGerald GA, Patrono C. The coxibs, selective inhibitors of cyclooxygenase‐2. New England Journal of Medicine 2001;345(6):433‐42. - PubMed
Graff 2007
-
- Graff J, Arabmotlagh M, Cheung R, Geisslinger G, Harder S. Effects of parecoxib and dipyrone on platelet aggregation in patients undergoing meniscectomy: a double‐blind, randomized, parallel‐group study. Clinical Therapeutics 2007;29(3):438‐47. - PubMed
Grahame‐Smith 2002
-
- Grahame‐Smith DG, Aronson JK. Oxford textbook of clinical pharmacology and drug therapy. 3rd Edition. Oxford: Oxford University Press, 2002. [ISBN: 13: 978‐0‐19‐263234‐0]
Hall 2008
Harris 2004
-
- Harris SI, Stoltz RR, LeComte D, Hubbard RC. Parecoxib sodium demonstrates gastrointestinal safety comparable to placebo in healthy subjects. Journal of Clinical Gastroenterology 2004;38(7):575‐80. - PubMed
Hawkey 1999
-
- Hawkey CJ. Cox‐2 inhibitors. Lancet 1999;353(9149):307‐14. - PubMed
Jadad 1996a
-
- Jadad A, Carroll D, Moore RA, McQuay HJ. Developing a database of published reports of randomised clinical trials in pain research. Pain 1996;66:239‐46. - PubMed
Jadad 1996b
-
- Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gavaghan DJ, McQuay HJ. Assessing the quality of reports of randomized clinical trials: is blinding necessary?. Controlled Clinical Trials 1996;17:1‐12. - PubMed
L'Abbé 1987
-
- L'Abbé KA, Detsky AS, O'Rourke K. Meta‐analysis in clinical research. Annals of Internal Medicine 1987;107:224‐33. - PubMed
Layton 2006
-
- Layton D, Marshall V, Boshier A, Friedmann P, Shakir SA. Serious skin reactions and selective COX‐2 inhibitors: a case series from prescription‐event monitoring in England. Drug Safety 2006;29(8):687‐96. - PubMed
McQuay 2005
Moher 1999
Moore 1996
-
- Moore A, McQuay H, Gavaghan D. Deriving dichotomous outcome measures from continuous data in randomised controlled trials of analgesics. Pain 1996;66(2‐3):229‐37. - PubMed
Moore 1997a
-
- Moore A, McQuay H, Gavaghan D. Deriving dichotomous outcome measures from continuous data in randomised controlled trials of analgesics: Verification from independent data. Pain 1997;69(1‐2):127‐30. - PubMed
Moore 1997b
-
- Moore A, Moore O, McQuay H, Gavaghan D. Deriving dichotomous outcome measures from continuous data in randomised controlled trials of analgesics: Use of pain intensity and visual analogue scales. Pain 1997;69(3):311‐5. - PubMed
Moore 1998
-
- Moore RA, Gavaghan D, Tramer M, Collins SL, McQuay HJ. Size is everything ‐ large amounts of information are needed to overcome random effects in estimating direction and magnitude of treatment effects. Pain 1998;73(3):209‐16. - PubMed
Moore 2003
-
- Moore RA, Edwards J, Barden J, McQuay HJ. Bandolier's Little Book of Pain. Oxford: Oxford University Press, 2003.
Moore 2005
-
- Moore RA, Edwards JE, McQuay HJ. Acute pain: individual patient meta‐analysis shows the impact of different ways of analysing and presenting results. Pain 2005;116(3):322‐31. - PubMed
Moore 2006
-
- Moore A, McQuay H. Bandolier's Little Book of Making Sense of the Medical Evidence. Oxford: Oxford University Press, 2006.
Moore 2008
Morris 1995
Noveck 2001
-
- Noveck RJ, Laurent A, Kuss M, Talwalker S, Hubbard RC. Parecoxib sodium does not impair platelet function in healthy elderly and non‐elderly individuals: Two randomised, controlled trials. Clinical Drug Investigation 2001;21(7):465‐76.
Nussmeier 2005
-
- Nussmeier NA, Whelton AA, Brown MT, Langford RM, Hoeft A, Parlow JL, et al. Complications of the COX‐2 inhibitors parecoxib and valdecoxib after cardiac surgery. New England Journal of Medicine 2005;352(11):1081‐91. - PubMed
Oldman 1999
Ott 2003
-
- Ott E, Nussmeier NA, Duke PC, Feneck RO, Alston RP, Snabes MC, et al. Efficacy and safety of the cyclooxygenase 2 inhibitors parecoxib and valdecoxib in patients undergoing coronary artery bypass surgery. Journal of Thoracic and Cardiovascular Surgery 2003;125(6):1481‐92. - PubMed
Roy 2007
Smith 2000
-
- Smith LA, Carroll D, Edwards JE, Moore RA, McQuay HJ. Single‐dose ketorolac and pethidine in acute postoperative pain: systematic review with meta‐analysis. British Journal of Anaesthesia 2000;84(1):48‐58. - PubMed
Stoltz 2002
-
- Stoltz RR, Harris SI, Kuss ME, LeComte D, Talwalker S, Dhadda S, et al. Upper GI mucosal effects of parecoxib sodium in healthy elderly subjects. American Journal of Gastroenterology 2002;97(1):65‐71. - PubMed
Toms 2008
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Research Materials