

A cost-effectiveness study of caesarean-section deliveries by clinical officers, general practitioners and obstetricians in Burkina Faso
- PMID: 19371433
- PMCID: PMC2672919
- DOI: 10.1186/1478-4491-7-34
A cost-effectiveness study of caesarean-section deliveries by clinical officers, general practitioners and obstetricians in Burkina Faso
Abstract
Background: The aim of this paper was to evaluate the effectiveness and cost-effectiveness of alternative training strategies for increasing access to emergency obstetric care in Burkina Faso.
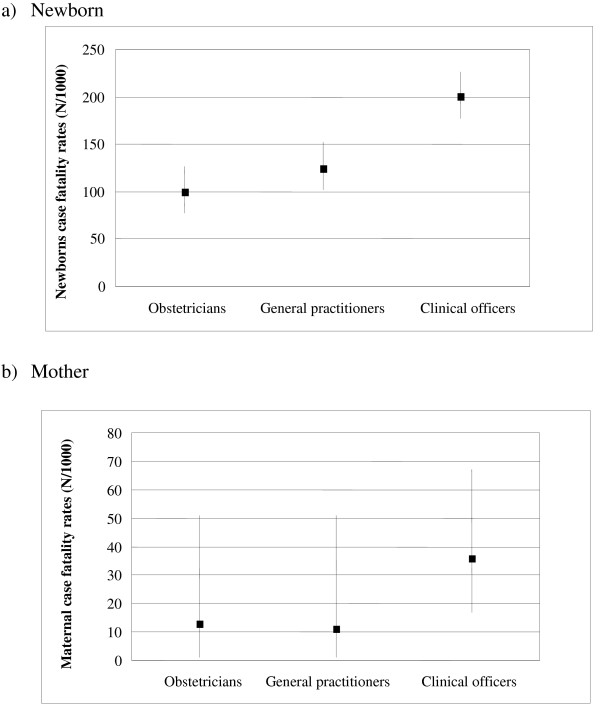
Methods: Case extraction forms were used to record data on 2305 caesarean sections performed in 2004 and 2005 in hospitals in six out of the 13 health regions of Burkina Faso. Main effectiveness outcomes were mothers' and newborns' case fatality rates. The costs of performing caesarean sections were estimated from a health system perspective and Incremental Cost-Effectiveness Ratios were computed using the newborn case fatality rates.
Results: Overall, case mixes per provider were comparable. Newborn case fatality rates (per thousand) varied significantly among obstetricians, general practitioners and clinical officers, at 99, 125 and 198, respectively. The estimated average cost per averted newborn death (x1000 live births) for an obstetrician-led team compared to a general practitioner-led team was 11,757 international dollars, and for a general practitioner-led team compared to a clinical officer-led team it was 200 international dollars. Training of general practitioners appears therefore to be both effective and cost-effective in the short run. Clinical officers are associated with a high newborn case fatality rate.
Conclusion: Training substitutes is a viable option to increase access to life-saving operations in district hospitals. The high newborn case fatality rate among clinical officers could be addressed by a refresher course and closer supervision. These findings may assist in addressing supply shortages of skilled health personnel in sub-Saharan Africa.
Figures
References
-
- Graham W. The Scandal of the Century. Br J Obstet Gynaecol. 1998;105:375–376. - PubMed
LinkOut - more resources
Full Text Sources
