

Continuous interscalene brachial plexus block via an ultrasound-guided posterior approach: a randomized, triple-masked, placebo-controlled study
- PMID: 19372355
- PMCID: PMC2745838
- DOI: 10.1213/ane.0b013e318199dc86
Continuous interscalene brachial plexus block via an ultrasound-guided posterior approach: a randomized, triple-masked, placebo-controlled study
Abstract
Background: The posterior approach for placing continuous interscalene catheters has not been studied in a controlled investigation. In this randomized, triple-masked, placebo-controlled study, we tested the hypothesis that an ultrasound-guided continuous posterior interscalene block provides superior postoperative analgesia compared to a single-injection ropivacaine interscalene block after moderately painful shoulder surgery.
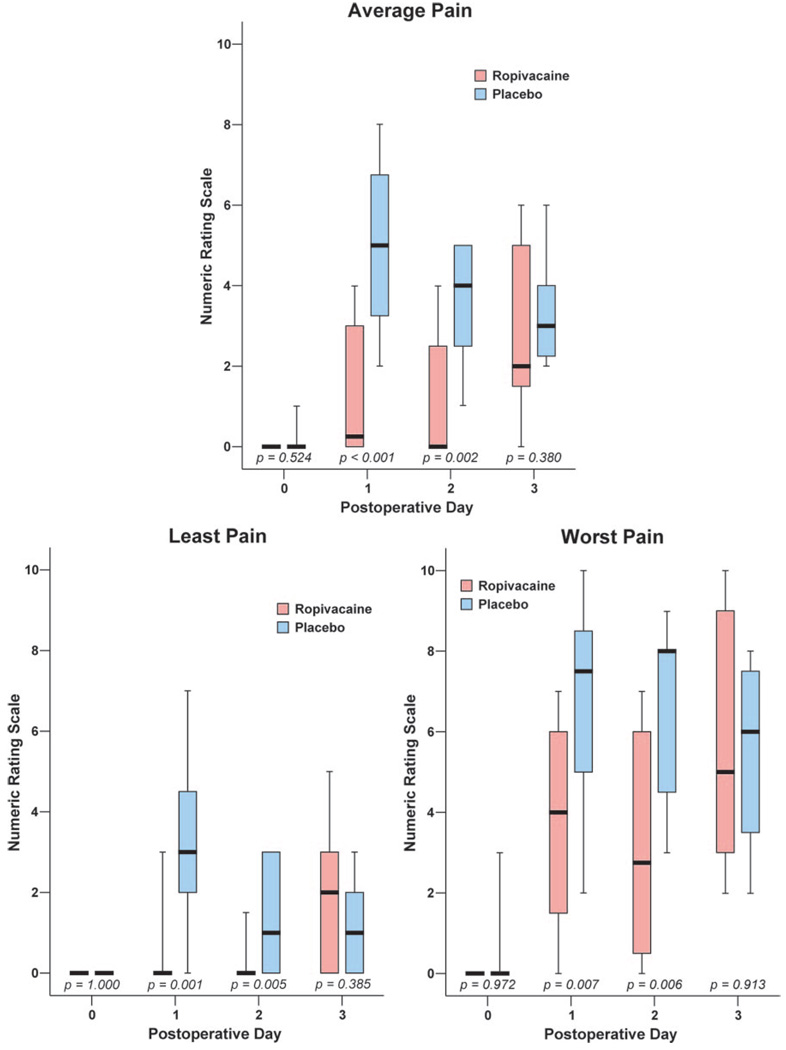
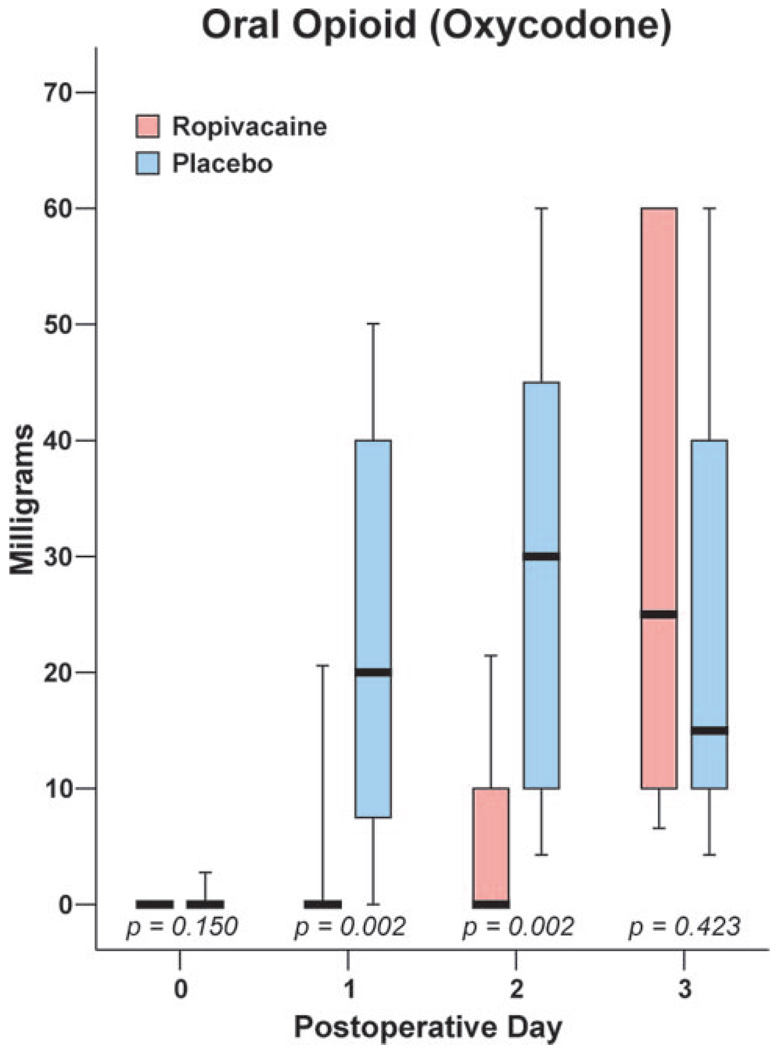
Methods: Preoperatively, subjects received a stimulating interscalene catheter using an ultrasound-guided, in-plane posterior approach. All subjects received an initial bolus of ropivacaine. Postoperatively, subjects were discharged with oral analgesics and a portable infusion device containing either ropivacaine 0.2% or normal saline programmed to deliver a perineural infusion over 2 days. The primary outcome was average pain on postoperative day (POD) 1 (scale: 0-10). Secondary outcomes included least and worst pain scores, oral opioid requirements, sleep disturbances, patient satisfaction, and incidence of complications.
Results: Of the 32 subjects enrolled, 30 perineural catheters were placed per protocol. Continuous ropivacaine perineural infusion (n = 15) produced a statistically and clinically significant reduction in average pain (median [10th-90th percentile]) on POD 1 compared with saline infusion (n = 15) after initial ropivacaine bolus (0.0 [0.0-5.0] versus 3.0 [0.0-6.0], respectively; P < 0.001). Median oral opioid consumption (oxycodone) was lower in the ropivacaine group than in the placebo group on POD 1 (P = 0.002) and POD 2 (P = 0.002). Subjects who received a ropivacaine infusion suffered fewer sleep disturbances than those in the placebo group (P = 0.005 on POD 0 and 1 nights) and rated their satisfaction with analgesia higher than subjects who received normal saline (P < 0.001).
Conclusions: Compared to a single-injection interscalene block, a 2-day continuous posterior interscalene block provides greater pain relief, minimizes supplemental opioid requirements, greatly improves sleep quality, and increases patient satisfaction after moderate-to-severe painful outpatient shoulder surgery.
Figures
References
-
- Klein SM, Grant SA, Greengrass RA, Nielsen KC, Speer KP, White W, Warner DS, Steele SM. Interscalene brachial plexus block with a continuous catheter insertion system and a disposable infusion pump. Anesth Analg. 2000;91:1473–1478. - PubMed
-
- Ilfeld BM, Morey TE, Wright TW, Chidgey LK, Enneking FK. Continuous interscalene brachial plexus block for postoperative pain control at home: a randomized, double-blinded, placebo-controlled study. Anesth Analg. 2003;96:1089–1095. - PubMed
-
- Ilfeld BM, Vandenborne K, Duncan PW, Sessler DI, Enneking FK, Shuster JJ, Theriaque DW, Chmielewski TL, Spadoni EH, Wright TW. Ambulatory continuous interscalene nerve blocks decrease the time to discharge readiness after total shoulder arthroplasty: a randomized, triple-masked, placebo-controlled study. Anesthesiology. 2006;105:999–1007. - PubMed
-
- Grant SA, Nielsen KC, Greengrass RA, Steele SM, Klein SM. Continuous peripheral nerve block for ambulatory surgery. Reg Anesth Pain Med. 2001;26:209–214. - PubMed
-
- Stevens MF, Werdehausen R, Golla E, Braun S, Hermanns H, Ilg A, Willers R, Lipfert P. Does interscalene catheter placement with stimulating catheters improve postoperative pain or functional outcome after shoulder surgery? A prospective, randomized and double-blinded trial. Anesth Analg. 2007;104:442–447. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
