

Subarachnoid hemorrhage and the distribution of drugs delivered into the cerebrospinal fluid. Laboratory investigation
- PMID: 19374502
- PMCID: PMC4762042
- DOI: 10.3171/2009.2.JNS081256
Subarachnoid hemorrhage and the distribution of drugs delivered into the cerebrospinal fluid. Laboratory investigation
Abstract
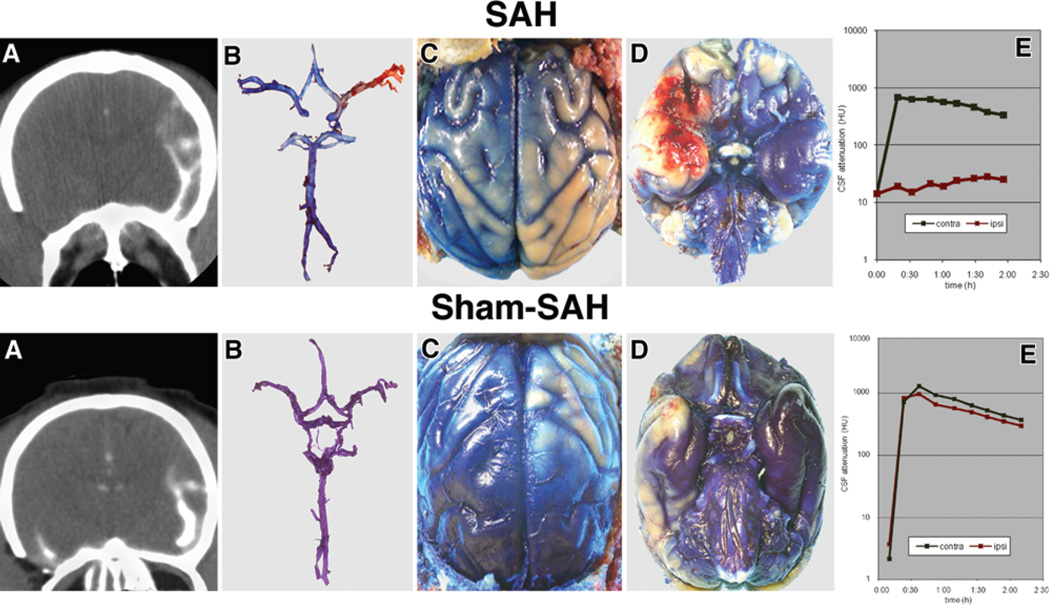
Object: Investigators in experimental and clinical studies have used the intrathecal route to deliver drugs to prevent or treat vasospasm. However, a clot near an artery or arteries after subarachnoid hemorrhage (SAH) may hamper distribution and limit the effects of intrathecally delivered compounds. In a primate model of right middle cerebral artery (MCA) SAH, the authors examined the distribution of Isovue-M 300 and 3% Evans blue after infusion into the cisterna magna CSF.
Methods: Ten cynomolgus monkeys were assigned to SAH and sham SAH surgery groups (5 in each group). Monkeys received CSF injections as long as 28 days after SAH and were killed 3 hours after the contrast/Evans blue injection. The authors assessed the distribution of contrast material on serial CT within 2 hours after contrast injection and during autopsy within 3 hours after Evans blue staining.
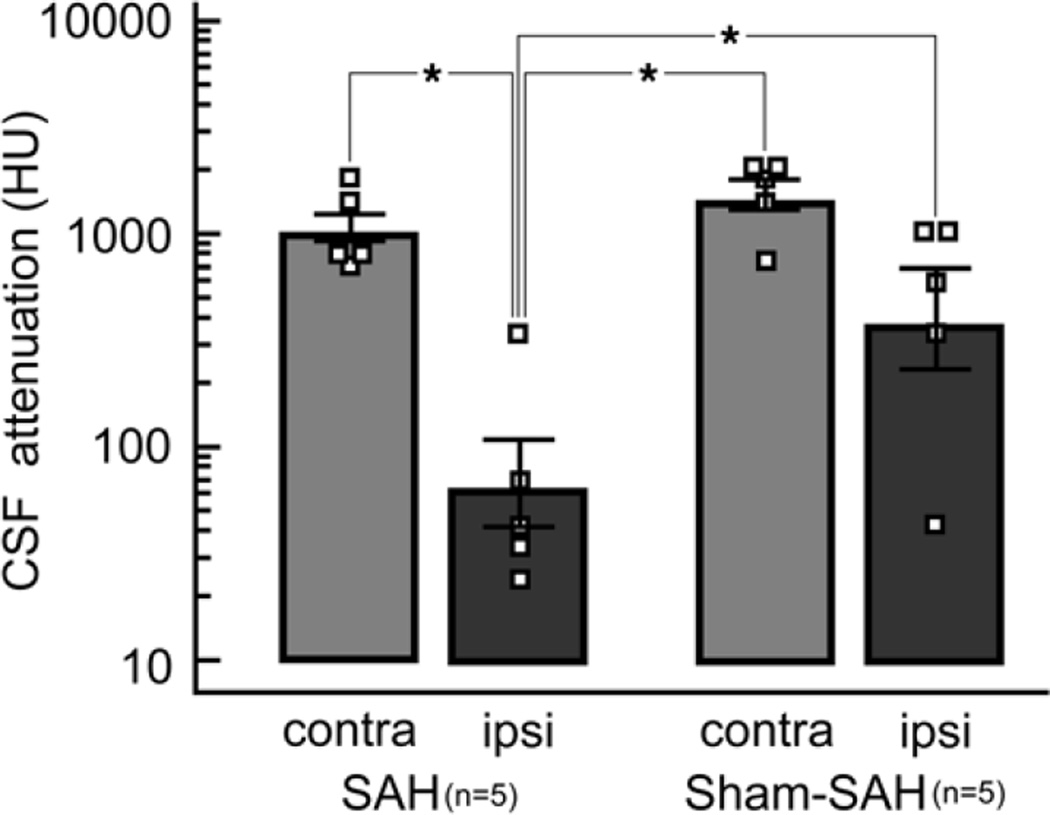
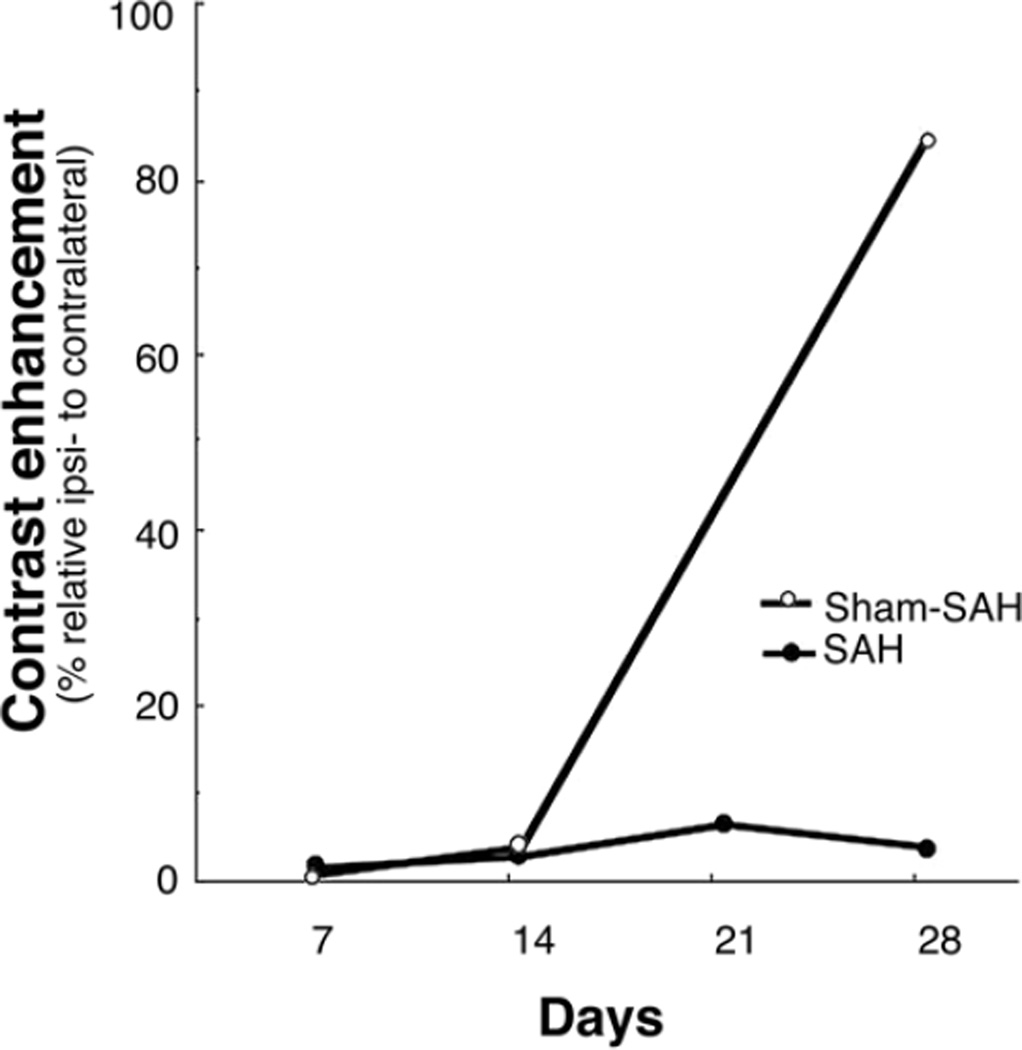
Results: Computed tomography cisternographies showed no contrast in the vicinity of the right MCA (p < 0.05 compared with left); the distribution of contrast surrounding the entire right cerebral hemisphere was substantially reduced. Postmortem analysis demonstrated much less Evans blue staining of the right hemisphere surface compared with the left. Furthermore, the Evans blue dye did not penetrate into the right sylvian fissure, which occurred surrounding the left MCA. The authors observed the same pattern of changes and differences in contrast distribution between SAH and sham SAH animals and between the right and the left hemispheres on Days 1, 3, 7, 14, 21, and 28 after SAH.
Conclusions: Intrathecal drug distribution is substantially limited by SAH. Thus, when using intrathecal drug delivery after SAH, vasoactive drugs are unlikely to reach the arteries that are at the highest risk of delayed cerebral vasospasm.
Figures
References
-
- Aihara Y, Jahromi BS, Yassari R, Sayama T, Macdonald RL. Effects of a nitric oxide donor on and correlation of changes in cyclic nucleotide levels with experimental vasospasm. Neurosurgery. 2003;52:661–667. - PubMed
-
- Amin-Hanjani S, Ogilvy C, Barker FII. Does intracisternal thrombolysis prevent vasospasm after aneurysmal subarachnoid hemorrhage? A meta-analysis. Neurosurgery. 2004;54:326–335. - PubMed
-
- Asano T, Sasaki T, Koide T, Takakura K, Sano K. Experimental evaluation of the beneficial effect of an antioxidant on cerebral vasospasm. Neurol Res. 1984;6:49–53. - PubMed
-
- Auer LM. Preventive nimodipine and acute aneurysm surgery. Heading for the control of complications after aneurysmal subarachnoid hemorrhage. Neurochirurgia (Stuttg) 1985;28:87–92. - PubMed
-
- Berg SL, Chamberlain MC. Current treatment of leptomeningeal metastases: systemic chemotherapy, intrathecal chemotherapy and symptom management. Cancer Treat Res. 2005;125:121–146. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
