

Rheological and physiological consequences of conversion of the maternal spiral arteries for uteroplacental blood flow during human pregnancy
- PMID: 19375795
- PMCID: PMC2697319
- DOI: 10.1016/j.placenta.2009.02.009
Rheological and physiological consequences of conversion of the maternal spiral arteries for uteroplacental blood flow during human pregnancy
Abstract
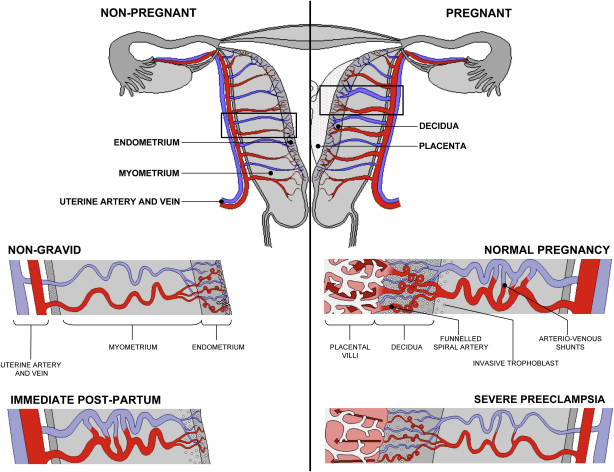
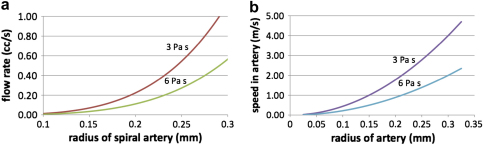
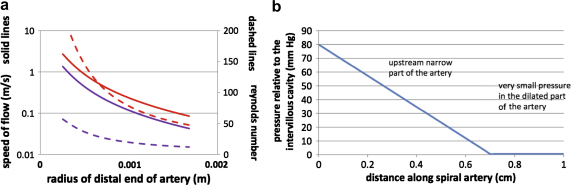
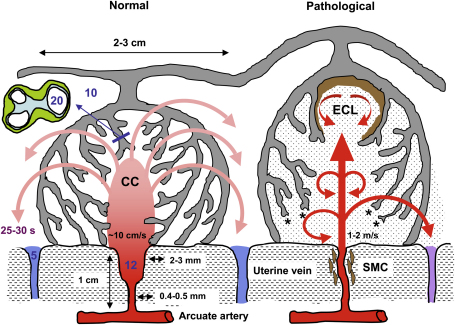
Physiological conversion of the maternal spiral arteries is key to a successful human pregnancy. It involves loss of smooth muscle and the elastic lamina from the vessel wall as far as the inner third of the myometrium, and is associated with a 5-10-fold dilation at the vessel mouth. Failure of conversion accompanies common complications of pregnancy, such as early-onset preeclampsia and fetal growth restriction. Here, we model the effects of terminal dilation on inflow of blood into the placental intervillous space at term, using dimensions in the literature derived from three-dimensional reconstructions. We observe that dilation slows the rate of flow from 2 to 3m/s in the non-dilated part of an artery of 0.4-0.5mm diameter to approximately 10 cm/s at the 2.5mm diameter mouth, depending on the exact radius and viscosity. This rate predicts a transit time through the intervillous space of approximately 25s, which matches observed times closely. The model shows that in the absence of conversion blood will enter the intervillous space as a turbulent jet at rates of 1-2m/s. We speculate that the high momentum will damage villous architecture, rupturing anchoring villi and creating echogenic cystic lesions as evidenced by ultrasound. The retention of smooth muscle will also increase the risk of spontaneous vasoconstriction and ischaemia-reperfusion injury, generating oxidative stress. Dilation has a surprisingly modest impact on total blood flow, and so we suggest the placental pathology associated with deficient conversion is dominated by rheological consequences rather than chronic hypoxia.
Figures
References
-
- Gordon M.C. Maternal physiology. In: Gabbe S.G., Niebyl J.R., Simpson J.L., editors. Obstetrics. Normal and problem pregnancies. Churchill Livingstone; Philadelphia: 2007. pp. 55–84.
-
- Clapp J.F., 3rd, Capeless E. Cardiovascular function before, during, and after the first and subsequent pregnancies. Am J Cardiol. 1997;80:1469–1473. - PubMed
-
- Khong T.Y., De Wolf F., Robertson W.B., Brosens I. Inadequate maternal vascular response to placentation in pregnancies complicated by pre-eclampsia and by small-for-gestational age infants. Br J Obstet Gynaecol. 1986;93:1049–1059. - PubMed
-
- Khong T.Y., Liddell H.S., Robertson W.B. Defective haemochorial placentation as a cause of miscarriage. A preliminary study. Br J Obstet Gynaecol. 1987;94:649–655. - PubMed
-
- Meekins J.W., Pijnenborg R., Hanssens M., McFadyen I.R., Van Assche F.A. A study of placental bed spiral arteries and trophoblast invasion in normal and severe pre-eclamptic pregnancies. Br J Obstet Gynaecol. 1994;101:669–674. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
