

Quality of life and economic outcomes with surgical ventricular reconstruction in ischemic heart failure: results from the Surgical Treatment for Ischemic Heart Failure trial
- PMID: 19376309
- PMCID: PMC2694042
- DOI: 10.1016/j.ahj.2009.03.008
Quality of life and economic outcomes with surgical ventricular reconstruction in ischemic heart failure: results from the Surgical Treatment for Ischemic Heart Failure trial
Abstract
Background: Surgical ventricular reconstruction (SVR) is used in conjunction with coronary artery bypass graft surgery (CABG) to improve left ventricular function and clinical outcomes in selected patients with ischemic heart failure. The impact of SVR on quality of life (QOL) and medical costs is unknown.
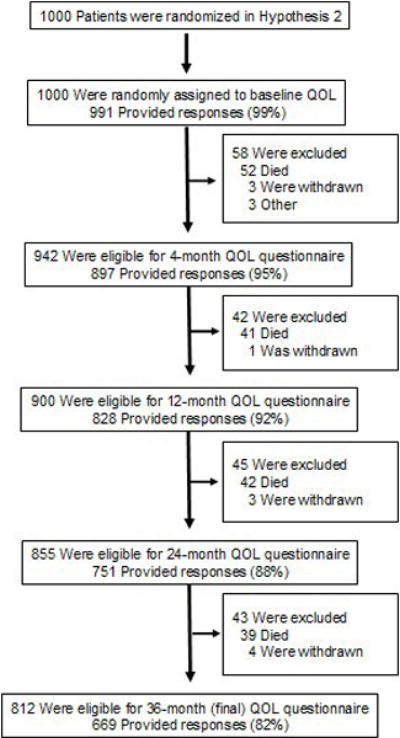
Methods: We compared CABG plus SVR with CABG alone in 1,000 patients with ischemic heart failure, an anterior wall scar, and a left ventricular ejection fraction <or=0.35. In 991 (99% of eligible), we collected a battery of QOL instruments. The principal, prespecified QOL measure was the Kansas City Cardiomyopathy Questionnaire, which evaluates the effects of heart failure symptoms on QOL using a scale from 0 to 100 with higher scores indicating better QOL. Structured QOL interviews were conducted at baseline, 4, 12, 24, and 36 months post randomization and were >or=92% complete. Cost data were collected on 196 (98%) of 200 patients enrolled in the United States.
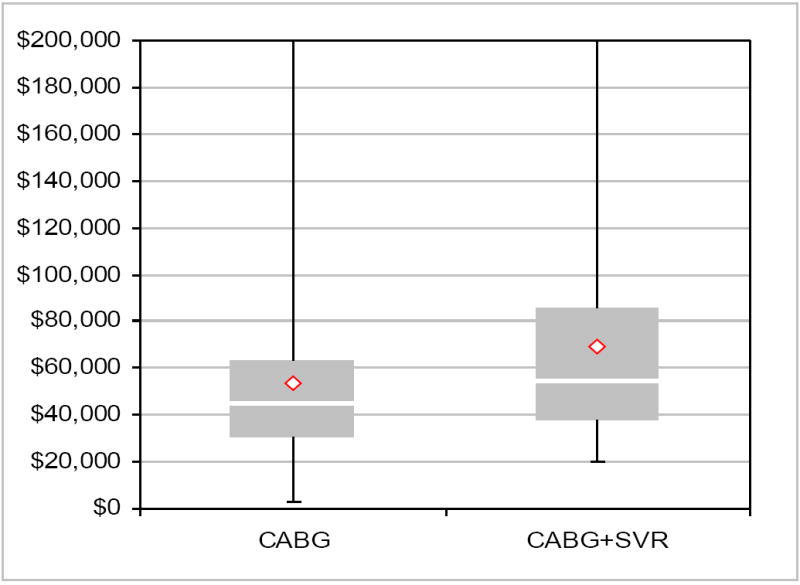
Results: Heart-failure-related QOL outcomes did not differ between the 2 treatment strategies out to 3 years (median Kansas City Cardiomyopathy Questionnaire scores for CABG alone and CABG plus SVR, respectively: baseline 53 versus 54, P = .53; 3 years 85 versus 84, P = .89). There were no treatment-related differences in other QOL measures. In the US patients, total index hospitalization costs averaged over $14,500 higher for CABG plus SVR (P = .004) due primarily to 4.2 extra postoperative, high-intensity care days in the hospital.
Conclusions: Addition of SVR to CABG in patients with ischemic heart failure did not improve QOL but significantly increased health care costs.
Trial registration: ClinicalTrials.gov NCT00023595.
Conflict of interest statement
Figures
References
-
- Dor V. Reconstructive left ventricular surgery for post-ischemic akinetic dilatation. Semin Thorac Cardiovasc Surg. 1997;9:139–45. - PubMed
-
- Athanasuleas CL, Buckberg GD, Stanley AW, Siler W, Dor V, Di DM, Menicanti L, meida de OS, Beyersdorf F, Kron IL, Suma H, Kouchoukos NT, Moore W, McCarthy PM, Oz MC, Fontan F, Scott ML, Accola KA. Surgical ventricular restoration in the treatment of congestive heart failure due to post-infarction ventricular dilation. J Am Coll Cardiol. 2004;44:1439–45. - PubMed
-
- Sartipy U, Albage A, Lindblom D. Improved health-related quality of life and functional status after surgical ventricular restoration. Ann Thorac Surg. 2007;83:1381–7. - PubMed
-
- Cotrufo M, Romano G, De Santo LS, Della CA, Amarelli C, Cafarella G, Maiello C, Scardone M. Treatment of extensive ischemic cardiomyopathy: quality of life following two different surgical strategies. Eur J Cardiothorac Surg. 2005;27:481–7. - PubMed
-
- Jones RH STICH Hypothesis 2 Investigators. Surgical Treatment for Ischemic Heart Failure (STICH) trial evaluation of surgical ventricular reconstruction. 2009 Submitted.
