

Branch retinal artery occlusion: natural history of visual outcome
- PMID: 19376586
- PMCID: PMC2759688
- DOI: 10.1016/j.ophtha.2009.01.015
Branch retinal artery occlusion: natural history of visual outcome
Abstract
Objective: To investigate systematically the natural history of visual outcome in branch retinal artery occlusion (BRAO).
Design: Cohort study.
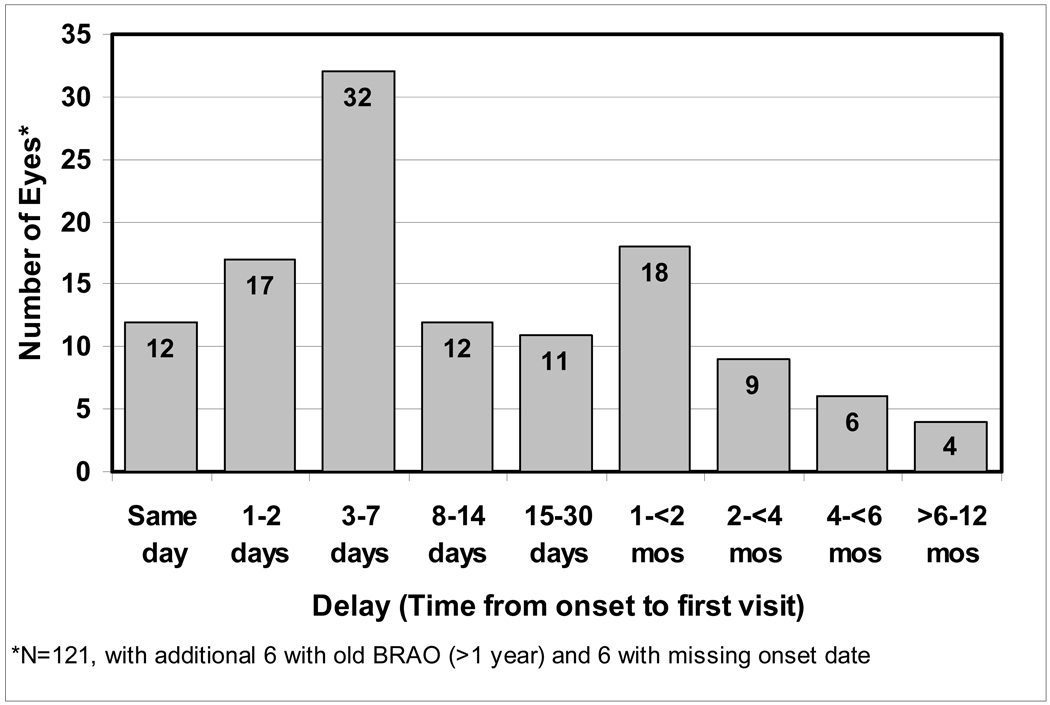
Participants: We included 199 consecutive untreated patients (212 eyes) with BRAO, first seen in our clinic from 1973 to 2000.
Methods: At first visit, all patients had a detailed ophthalmic and medical history, and comprehensive ophthalmic evaluation. Visual evaluation was done by recording visual acuity, using the Snellen visual acuity chart, and visual fields with a Goldmann perimeter. The same ophthalmic evaluation was performed at each follow-up visit.
Main outcome measures: Visual acuity and visual fields.
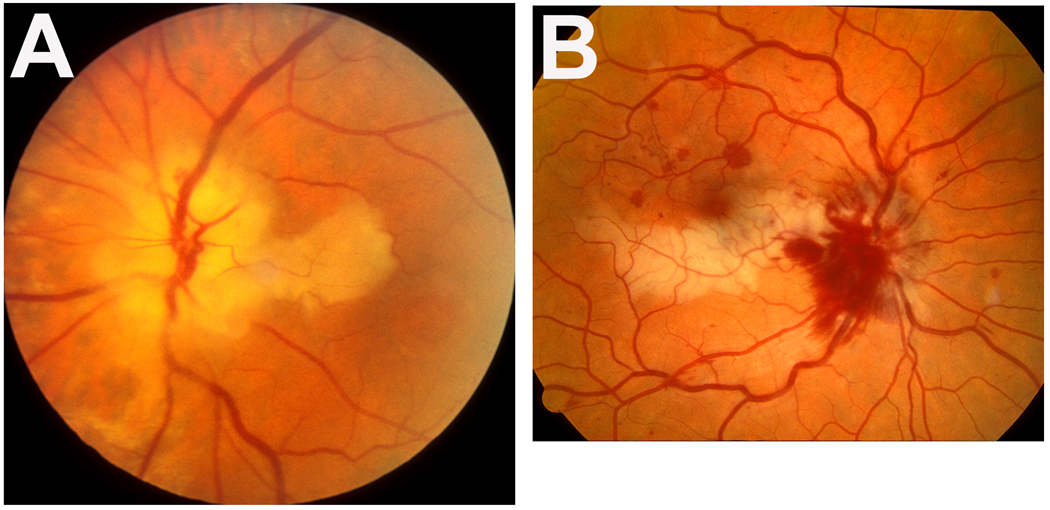
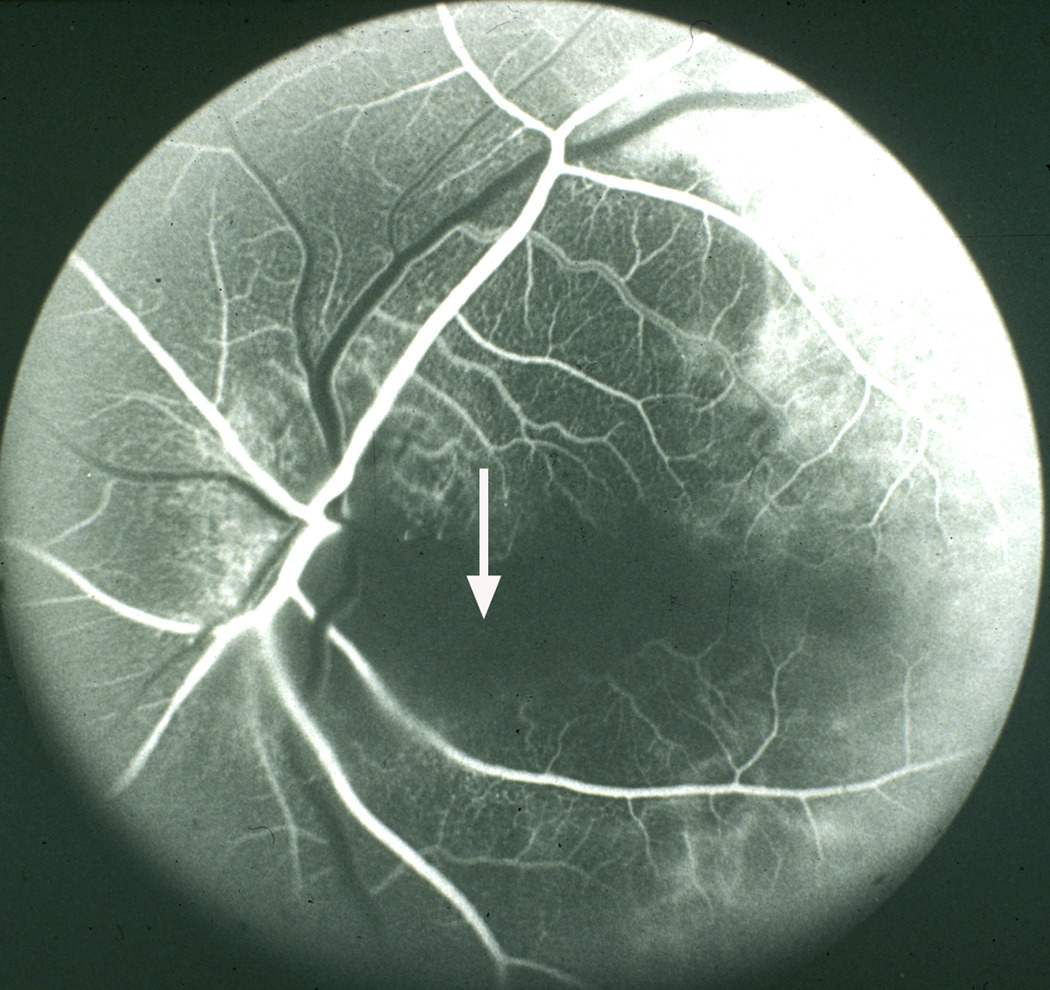
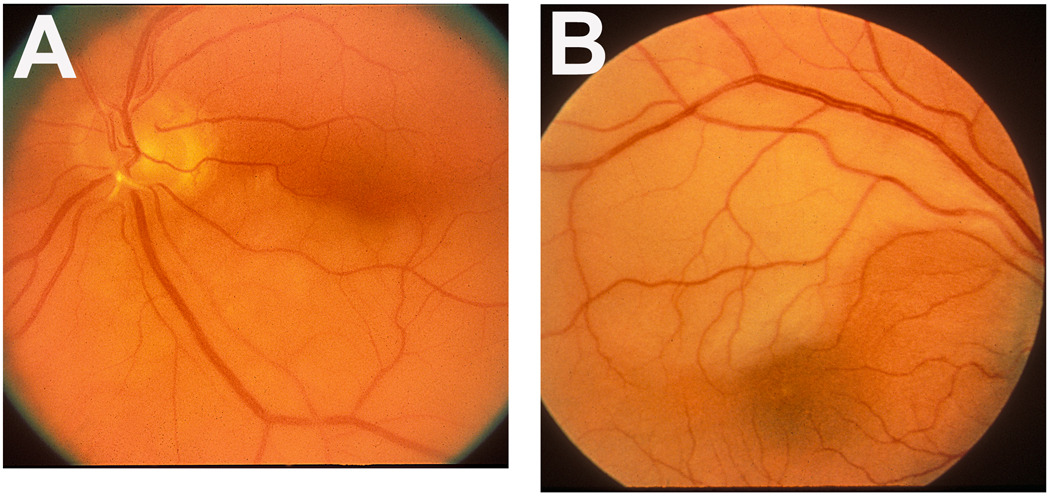
Results: We classified BRAO into permanent (133 eyes) and transient (18 eyes) and cilioretinal artery occlusion (CLRAO; 61 eyes). In eyes with permanent BRAO, of the 61 eyes seen within 7 days of onset, initial visual acuity was >or=20/40 in 74%, central scotoma in 20%, central inferior altitudinal defect in 13%, and inferior nasal and superior sector defects in 29% and 24%, respectively. Of those with follow-up, in the eyes with visual acuity <20/40, it improved in 79% (11/14), abnormal central visual field defect improved in 47%, and abnormal peripheral visual field defect improved in 52%. Of the 18 eyes with transient BRAO, initially 17 (94%) had visual acuity of >or=20/40 and 1 (6%) <20/40, which improved to 20/30 on follow-up. Of the 11 eyes with nonarteritic CLRAO alone, visual acuity was <20/40 in 3 eyes, which improved to >or=20/40 in all during follow-up. In CLRAO on follow-up of 9 eyes, the central field improved in 4. When CLRAO was associated with retinal vein occlusion (38 eyes) or giant cell arteritis (12 eyes), visual findings were influenced by the associated diseases.
Conclusions: These findings show that a visual acuity of >or=20/40 is seen initially in 74% of cases of permanent BRAO, 94% of transient BRAO, and 73% of nonarteritic CLRAO alone; and finally on follow-up, in 89%, 100%, and 100% of cases, respectively. The effectiveness of various treatment modalities for visual outcome has to be judged against this background.
Financial disclosure(s): The authors have no proprietary or commercial interest in any materials discussed in this article.
Conflict of interest statement
The authors have no conflict of interest.
Figures
References
-
- Hayreh SS, Podhajsky P. Ocular neovascularization with retinal vascular occlusion II. Occurrence in central and branch retinal artery occlusion. Arch Ophthalmol. 1982;100:1585–1596. - PubMed
-
- Yuzurihara D, Iijima H. Visual outcome in central retinal and branch retinal artery occlusion. Jpn J Ophthalmol. 2004;48:490–492. - PubMed
-
- Mason JO, Shah AA, Vail RS, et al. Branch retinal artery occlusion: visual prognosis. Am J Ophthalmol. 2008;46:455–457. - PubMed
-
- Hayreh SS, Zimmerman B. Central retinal artery occlusion: visual outcome. Am J Ophthalmol. 2005;140:376–391. - PubMed
-
- Hayreh SS, Zimmerman MB. Fundus changes in central retinal artery occlusion. Retina. 2007;27:276–289. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
