

Neostigmine decreases bupivacaine use by patient-controlled epidural analgesia during labor: a randomized controlled study
- PMID: 19377050
- PMCID: PMC2843405
- DOI: 10.1213/ane.0b013e31819518e4
Neostigmine decreases bupivacaine use by patient-controlled epidural analgesia during labor: a randomized controlled study
Abstract
Background: Intrathecal neostigmine not only produces analgesia but also severe nausea. In contrast, epidural neostigmine enhances opioid and local anesthetic analgesia without causing nausea. Previous studies examined only single epidural neostigmine bolus administration and did not assess the efficacy of continuous epidural infusion or several aspects of maternal and fetal safety. We therefore tested the hypothesis that epidural neostigmine in combination with bupivacaine by continuous infusion during labor would reduce the amount of bupivacaine required.
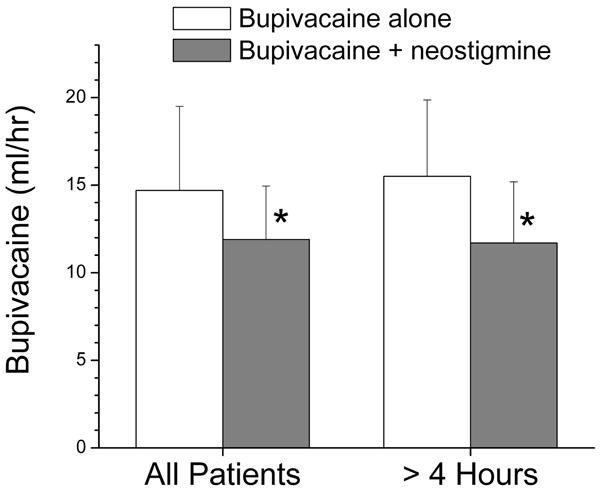
Methods: Twelve healthy women scheduled for elective cesarean delivery were assigned to receive epidural neostigmine, 40 microg (first six subjects) or 80 microg (second six subjects) as a single bolus, with fetal heart rate (FHR) and uterine contractions monitored for 20 min. In a subsequent experiment, 40 healthy laboring women were randomized to receive bupivacaine 1.25 mg/mL alone or with neostigmine 4 microg/mL by patient-controlled epidural analgesia. The primary outcome measure was hourly bupivacaine use.
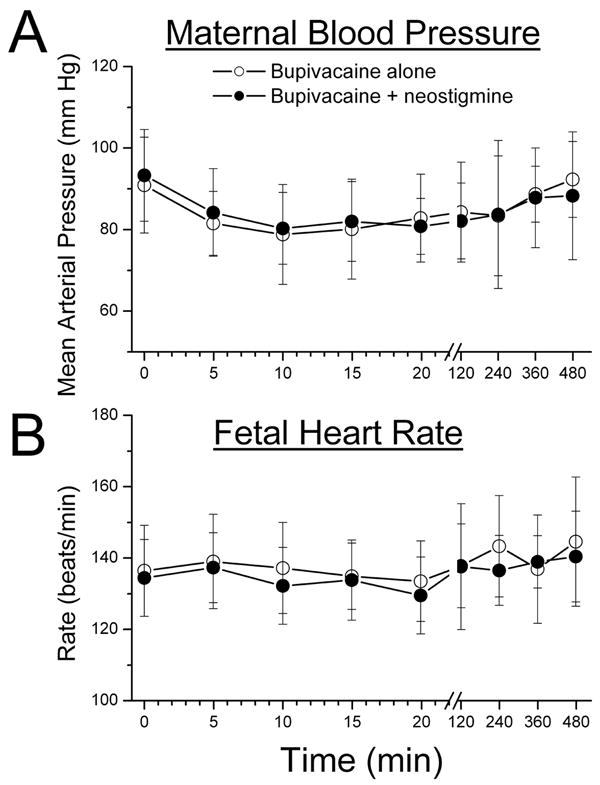
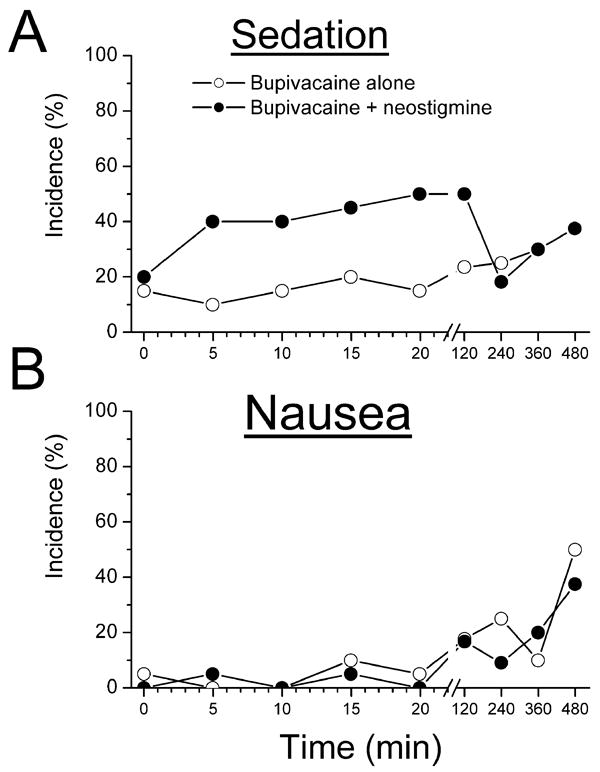
Results: Epidural neostigmine bolus did not alter baseline FHR, induce contractions, or produce nausea. Epidural neostigmine infusion reduced bupivacaine requirement by 19% in all patients and 25% in those with >4 h of treatment (P < 0.05 for both) but might have contributed to the incidence of mild sedation. Mode of delivery, incidence of maternal nausea, and FHR abnormality were similar between groups.
Conclusions: These data show that adding epidural neostigmine 4 microg/mL reduces the hourly bupivacaine requirement by 19%-25% with patient-controlled epidural analgesia during labor. Administered as a bolus and by continuous infusion at the studied doses, epidural neostigmine does not cause nausea and does not induce uterine contractions or FHR abnormalities, but mild sedation can occur.
Figures
Comment in
-
Clinical investigation of neuraxially administered drugs: a regulatory perspective.Anesth Analg. 2009 Aug;109(2):299-300. doi: 10.1213/ane.0b013e3181a801b9. Anesth Analg. 2009. PMID: 19608794 No abstract available.
Similar articles
-
Epidural Neostigmine versus Fentanyl to Decrease Bupivacaine Use in Patient-controlled Epidural Analgesia during Labor: A Randomized, Double-blind, Controlled Study.Anesthesiology. 2017 Jul;127(1):50-57. doi: 10.1097/ALN.0000000000001669. Anesthesiology. 2017. PMID: 28475555 Clinical Trial.
-
Intrathecal sufentanil and fetal heart rate abnormalities: a double-blind, double placebo-controlled trial comparing two forms of combined spinal epidural analgesia with epidural analgesia in labor.Anesth Analg. 2004 Apr;98(4):1153-1159. doi: 10.1213/01.ANE.0000101980.34587.66. Anesth Analg. 2004. PMID: 15041616 Clinical Trial.
-
Epidural neostigmine produces analgesia but also sedation in women after cesarean delivery.Anesthesiology. 2004 Feb;100(2):381-5. doi: 10.1097/00000542-200402000-00030. Anesthesiology. 2004. PMID: 14739815 Clinical Trial.
-
Low-dose clonidine and neostigmine prolong the duration of intrathecal bupivacaine-fentanyl for labor analgesia.Anesthesiology. 2000 Feb;92(2):361-6. doi: 10.1097/00000542-200002000-00016. Anesthesiology. 2000. PMID: 10691221 Clinical Trial.
-
Efficacy of Intrathecal Fentanyl for Cesarean Delivery: A Systematic Review and Meta-analysis of Randomized Controlled Trials With Trial Sequential Analysis.Anesth Analg. 2020 Jan;130(1):111-125. doi: 10.1213/ANE.0000000000003975. Anesth Analg. 2020. PMID: 30633056
Cited by
-
Optimal single-dose epidural neostigmine for postoperative analgesia after partial hepatectomy.Indian J Pharmacol. 2014 Nov-Dec;46(6):613-6. doi: 10.4103/0253-7613.144918. Indian J Pharmacol. 2014. PMID: 25538332 Free PMC article. Clinical Trial.
-
Postoperative analgesic effect of epidural neostigmine following caesarean section.Hippokratia. 2014 Jan;18(1):44-9. Hippokratia. 2014. PMID: 25125952 Free PMC article.
-
Can Epidural Dexamethasone Reduce Patient-Controlled Epidural Consumption of Fentanyl and Levobupivacaine in Laboring Women? A Double-Blind, Randomized, Placebo-Controlled Trial.J Obstet Gynaecol India. 2019 Jun;69(3):258-265. doi: 10.1007/s13224-018-1189-2. Epub 2018 Nov 22. J Obstet Gynaecol India. 2019. PMID: 31178642 Free PMC article.
-
Comparison between the intravenous and caudal routes of sufentanil in children undergoing orchidopexy and further evaluation of the association of caudal adrenaline and neostigmine.Saudi J Anaesth. 2014 Jul;8(3):345-50. doi: 10.4103/1658-354X.136430. Saudi J Anaesth. 2014. PMID: 25191184 Free PMC article.
-
Epidural Infusion of Morphine and Levobupivacaine through a Subcutaneous Port for Cancer Pain Management.Korean J Pain. 2014 Apr;27(2):139-44. doi: 10.3344/kjp.2014.27.2.139. Epub 2014 Mar 28. Korean J Pain. 2014. PMID: 24748942 Free PMC article.
References
-
- Sharma SK, McIntire DD, Wiley J, Leveno KJ. Labor analgesia and cesarean delivery: an individual patient meta-analysis of nulliparous women. Anesthesiology. 2004;100:142–8. - PubMed
-
- Lyak SZ, Eisenach JC, Dobson CE. Patient controlled analgesia during labor. A comparison of three solutions with a continuous infusion control. Anesthesiology. 1990;72:44–49. - PubMed
-
- Benhamou D. Are local anesthetics needed for local anesthesia? Anesthesiology. 2004;101:271–2. - PubMed
-
- Yaksh TL, Dirksen R, Harty GJ. Antionocieptive effects of intrathecally injected cholinomimetric drugs in rat and cat. Eur Journal of Pharm. 1985;117:81–88. - PubMed
-
- Yaksh TL, Grafe MR, Malkmus S, Rathbun ML, Eisenach JC. Studies on the safety of chronically administered intrathecal neostigmine methylsulfate in rats and dogs. Anesthesiology. 1995;82:412–427. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
