

Unrecognized non-Q-wave myocardial infarction: prevalence and prognostic significance in patients with suspected coronary disease
- PMID: 19381280
- PMCID: PMC2661255
- DOI: 10.1371/journal.pmed.1000057
Unrecognized non-Q-wave myocardial infarction: prevalence and prognostic significance in patients with suspected coronary disease
Abstract
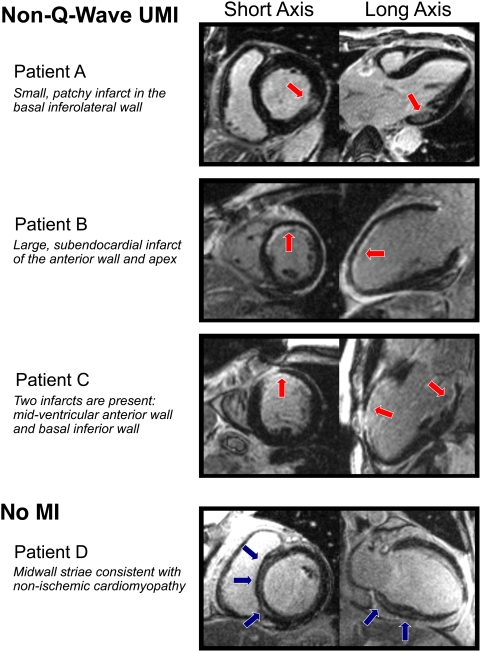
Background: Unrecognized myocardial infarction (UMI) is known to constitute a substantial portion of potentially lethal coronary heart disease. However, the diagnosis of UMI is based on the appearance of incidental Q-waves on 12-lead electrocardiography. Thus, the syndrome of non-Q-wave UMI has not been investigated. Delayed-enhancement cardiovascular magnetic resonance (DE-CMR) can identify MI, even when small, subendocardial, or without associated Q-waves. The aim of this study was to investigate the prevalence and prognosis associated with non-Q-wave UMI identified by DE-CMR.
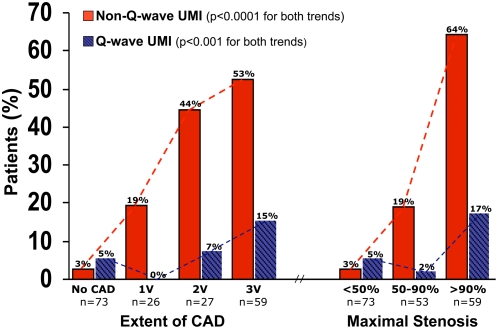
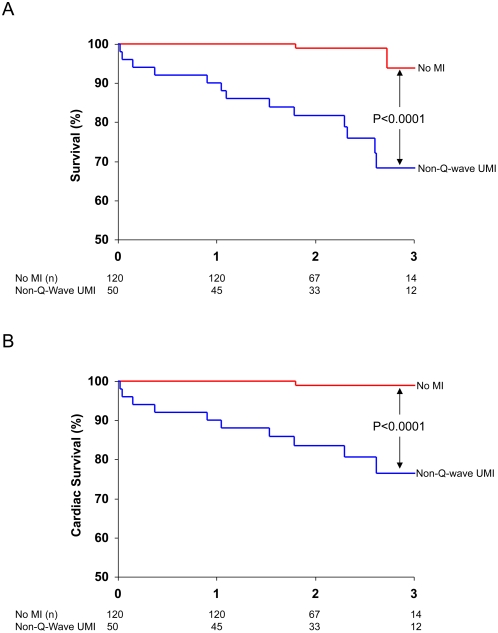
Methods and findings: We conducted a prospective study of 185 patients with suspected coronary disease and without history of clinical myocardial infarction who were scheduled for invasive coronary angiography. Q-wave UMI was determined by electrocardiography (Minnesota Code). Non-Q-wave UMI was identified by DE-CMR in the absence of electrocardiographic Q-waves. Patients were followed to determine the prognostic significance of non-Q-wave UMI. The primary endpoint was all-cause mortality. The prevalence of non-Q-wave UMI was 27% (50/185), compared with 8% (15/185) for Q-wave UMI. Patients with non-Q-wave UMI were older, were more likely to have diabetes, and had higher Framingham risk than those without MI, but were similar to those with Q-wave UMI. Infarct size in non-Q-wave UMI was modest (8%+/-7% of left ventricular mass), and left ventricular ejection fraction (LVEF) by cine-CMR was usually preserved (52%+/-18%). The prevalence of non-Q-wave UMI increased with the extent and severity of coronary disease on angiography (p<0.0001 for both). Over 2.2 y (interquartile range 1.8-2.7), 16 deaths occurred: 13 in non-Q-wave UMI patients (26%), one in Q-wave UMI (7%), and two in patients without MI (2%). Multivariable analysis including New York Heart Association class and LVEF demonstrated that non-Q-wave UMI was an independent predictor of all-cause mortality (hazard ratio [HR] 11.4, 95% confidence interval [CI] 2.5-51.1) and cardiac mortality (HR 17.4, 95% CI 2.2-137.4).
Conclusions: In patients with suspected coronary disease, the prevalence of non-Q-wave UMI is more than 3-fold higher than Q-wave UMI. The presence of non-Q-wave UMI predicts subsequent mortality, and is incremental to LVEF.
Trial registration: Clinicaltrials.gov NCT00493168.
Conflict of interest statement
RJK and RMJ are inventors of a US patent on Delayed Enhancement CMR, which is owned by Northwestern University. No other potential conflict of interest relevant to this article was reported.
Figures
Comment in
-
What is the significance of unrecognized non-Q-wave myocardial infarction?PLoS Med. 2009 Apr 21;6(4):e1000060. doi: 10.1371/journal.pmed.1000060. Epub 2009 Apr 21. PLoS Med. 2009. PMID: 19381282 Free PMC article.
-
Detecting unrecognized myocardial infarction: the importance of imaging.Curr Cardiol Rep. 2010 Jan;12(1):3-5. doi: 10.1007/s11886-009-0079-8. Curr Cardiol Rep. 2010. PMID: 20425177 Free PMC article. No abstract available.
References
-
- Kannel WB, Abbott RD. Incidence and prognosis of unrecognized myocardial infarction. An update on the Framingham study. N Engl J Med. 1984;311:1144–1147. - PubMed
-
- Sheifer SE, Gersh BJ, Yanez ND, 3rd, Ades PA, Burke GL, et al. Prevalence, predisposing factors, and prognosis of clinically unrecognized myocardial infarction in the elderly. J Am Coll Cardiol. 2000;35:119–126. - PubMed
-
- Sigurdsson E, Thorgeirsson G, Sigvaldason H, Sigfusson N. Unrecognized myocardial infarction: epidemiology, clinical characteristics, and the prognostic role of angina pectoris. The Reykjavik Study. Ann Intern Med. 1995;122:96–102. - PubMed
-
- Gopinath N, Kaul U, Chadha SL, Sood AK, Bhattacharya D, et al. Asymptomatic coronary heart disease detected on epidemiological survey of urban population of Delhi. Indian Heart J. 1992;44:95–98. - PubMed
-
- Medalie JH, Goldbourt U. Unrecognized myocardial infarction: five-year incidence, mortality, and risk factors. Ann Intern Med. 1976;84:526–531. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
