

Red blood cell transfusion practices in acute lung injury: what do patient factors contribute?
- PMID: 19384204
- PMCID: PMC2729062
- DOI: 10.1097/CCM.0b013e3181a0022d
Red blood cell transfusion practices in acute lung injury: what do patient factors contribute?
Abstract
Objective: To describe red blood cell (RBC) transfusion practices and evaluate the association between patient-related factors and pretransfusion hemoglobin concentration in acute lung injury (ALI).
Design: Secondary analysis of prospectively collected data.
Setting: Nine intensive care units (ICUs) in three teaching hospitals in Baltimore, MD.
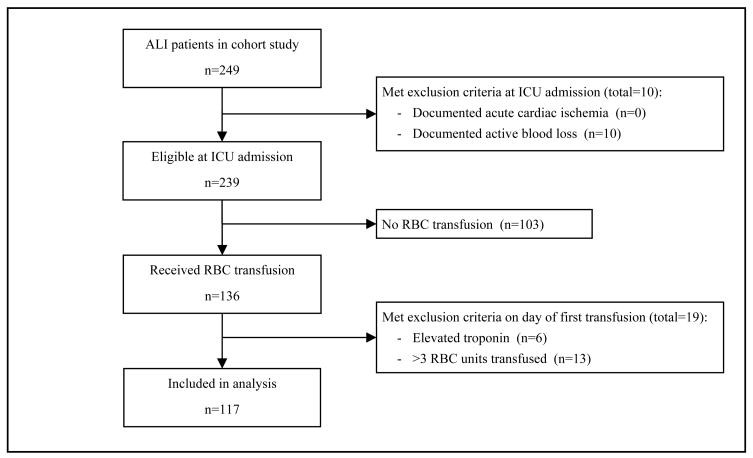
Patients: Two hundred forty-nine consecutive patients with ALI requiring mechanical ventilation.
Interventions: None.
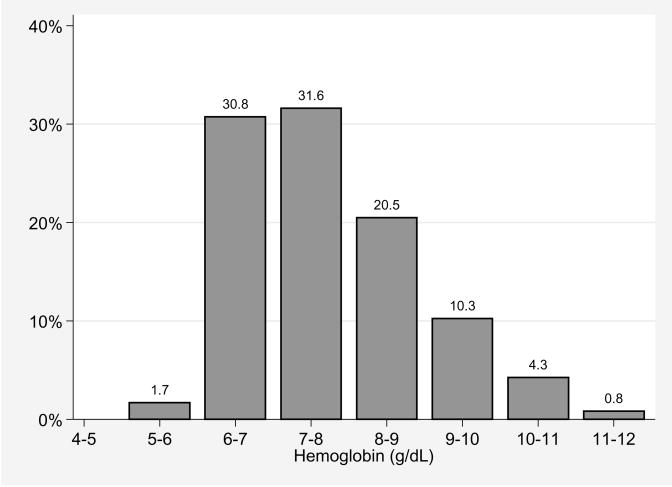
Measurements and main results: Simple and multiple linear regression analyses were used to evaluate the association between the nadir hemoglobin concentration on the day of initial RBC transfusion and 20 patient-level demographic, clinical and ICU treatment factors as well as ICU type. Of 249 patients with ALI, 47% received an RBC transfusion in the ICU without evidence of active hemorrhage or acute cardiac ischemia. The mean (sd) nadir hemoglobin on the day of first transfusion was 7.7 (1.1) g/dL with 67%, 36%, 15%, and 5% of patients transfused at >7, >8, >9, and >10 g/dL, respectively. Transfused patients received a mean (sd) of 5 (6) RBC units from ALI diagnosis to ICU discharge. Prehospital use of iron or erythropoietin and platelet transfusion in the ICU were independently associated with lower pretransfusion hemoglobin concentrations. No patient factors were associated with higher hemoglobin concentrations. Admission to a surgical (vs. medical) ICU was independently associated with a 0.6 g/dL (95% confidence interval 0.1-1.1 g/dL) higher pretransfusion hemoglobin.
Conclusions: Patients with ALI commonly receive RBC transfusions in the ICU. The pretransfusion hemoglobin observed in our study was lower than earlier studies, but a restrictive strategy was not universally adopted. Patient factors do not explain the gap between clinical trial evidence and routine transfusion practices. Future studies should further explore ICU- and physician-related factors as a source of variability in transfusion practice.
Figures
Comment in
-
Red blood cell transfusion in the critically ill: when is it time to say enough?Crit Care Med. 2009 Jun;37(6):2114-6. doi: 10.1097/CCM.0b013e3181a5c1f1. Crit Care Med. 2009. PMID: 19448462 No abstract available.
References
-
- Hebert PC, Wells G, Blajchman MA, et al. A multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med. 1999;340(6):409–417. - PubMed
-
- Duggan J, O’Connell D, Heller R, et al. Causes of hospital-acquired septicaemia--a case control study. Q J Med. 1993;86(8):479–483. - PubMed
-
- Taylor RW, Manganaro L, O’Brien J, et al. Impact of allogenic packed red blood cell transfusion on nosocomial infection rates in the critically ill patient. Crit Care Med. 2002;30(10):2249–2254. - PubMed
-
- Taylor RW, O’Brien J, Trottier SJ, et al. Red blood cell transfusions and nosocomial infections in critically ill patients. Crit Care Med. 2006;34(9):2302–2308. quiz 2309. - PubMed
-
- Shorr AF, Duh MS, Kelly KM, et al. Red blood cell transfusion and ventilator-associated pneumonia: A potential link? Crit Care Med. 2004;32(3):666–674. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
