

A treatment protocol for abdomino-pelvic injuries
- PMID: 19384622
- PMCID: PMC2656964
- DOI: 10.1007/s10195-008-0003-9
A treatment protocol for abdomino-pelvic injuries
Abstract
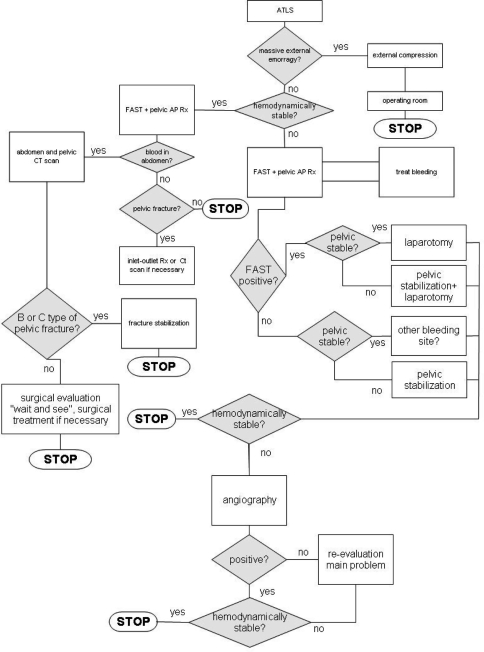
Background: Abdomino-pelvic injuries often present a challenge for the emergency department. Although literature reports several protocols on the treatment of abdomino-pelvic injuries aiming at defining the most advisable treatment line, optimal treatment is still controversial. This paper describes a protocol that has been used to treat abdomino-pelvic injuries in our hospital since 2002.
Materials and methods: In literature different protocol of abdomino-pelvic injuries are described and comparing them most of the difference are the timing of CT scan, the angiography and the laparotomy when treating a lesion of pelvic ring. If patient is haemodynamically instable and presents a lesion of pelvic ring our protocol suggest the simplest and fastest stabilization (pelvic external fixator) in emergency room and delay exam such as CT scan as second level exam. In the presence of an abdominal injury, with a positive focused assessment with sonography for trauma test, the first step should be a pelvic ring stabilization, as laparotomy decreases the abdominal pressure and reduces the tamponade effect on the retroperitoneum. According to presented protocol the angiography is not be a first choice treatment. This protocol was applied to 58 cases of abdomino-pelvic injury with unstable pelvic lesions from October 2002 to December 2005. Mean injury severity score was 27.2 (CI 24.1-30.3).
Results: Five patients (8%) died, three due to haemorrhagic shock and two due to pulmonary embolization. Four patients (6.9%) had a partial or complete cauda equina syndrome, four patients (6.9%) complained of mild incontinence, whilst 1 (1.7%) complained of urinary retention with multiple cystitis. Two patients (3.4%) with retention and multiple cystitis, had a malunion and a painful non-union of the fracture. Seven patients (12.3%) had neurological impairment: 5 (8.6%) sciatic nerve palsy, 1 (1.7%) lumbosacral root lesions in a C2-type fracture and there was one case (1.7%) of inconstant lumbago with sciatic pain. Twelve patients reported different levels of sexual dysfunction (20.7%).
Conclusions: Although validation with a larger cohort is required, our preliminary clinical data are similar to, or better than, those reported in the most recent publications on this question, suggesting that this protocol could well reduce both the mortality rate and the long term complications of abdominopelvic injuries.
Figures
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '9314298', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9314298/'}]}
- Agolini SF, Shah K, Jaffe J, Newcomb J, Rhodes M, Reed JF (1997) Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage. J Trauma 43:395–399 - PubMed
-
- Alonso M, Brathwaite C, Garcia V, Patterson L, Scherer T, Stafford P, Young J. East Practice Management Guidelines Work Group: practice management guidelines for the nonoperative management of blunt injury to the liver and spleen
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '9731815', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/9731815/'}]}
- Bassam D, Cephas GA, Ferguson KA, Beard LN, Young JS (1998) A protocol for the initial management of unstable pelvic fractures. Am Surg 64:862–867 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1097/00000658-200106000-00015', 'is_inner': False, 'url': 'https://doi.org/10.1097/00000658-200106000-00015'}, {'type': 'PMC', 'value': 'PMC1421328', 'is_inner': False, 'url': 'https://pmc.ncbi.nlm.nih.gov/articles/PMC1421328/'}, {'type': 'PubMed', 'value': '11407336', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/11407336/'}]}
- Biffl WL, Smith WR, Moore EE, Gonzalez RJ, Morgan SJ, Hennessey T, Offner PJ, Ray CE Jr, Franciose RJ, Burch JM (2001) Evolution of a multidisciplinary clinical pathway for the management of unstable patients with pelvic fractures. Ann Surg 233(6):843–850 - PMC - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/S0020-1383(03)00292-4', 'is_inner': False, 'url': 'https://doi.org/10.1016/s0020-1383(03)00292-4'}, {'type': 'PubMed', 'value': '14728948', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/14728948/'}]}
- Bircher M, Giannoudis PV (2004) Pelvic trauma management within the UK: a reflection of a failing trauma service. Injury 35(1):2–6 - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous
