

2008 Landis Award lecture. Inflammation and the autodigestion hypothesis
- PMID: 19384726
- PMCID: PMC2677689
- DOI: 10.1080/10739680902801949
2008 Landis Award lecture. Inflammation and the autodigestion hypothesis
Abstract
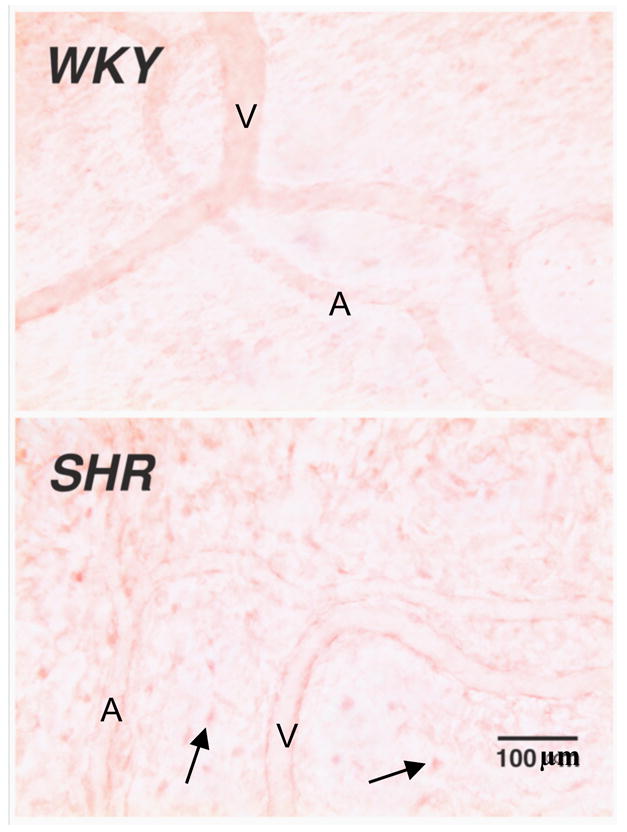
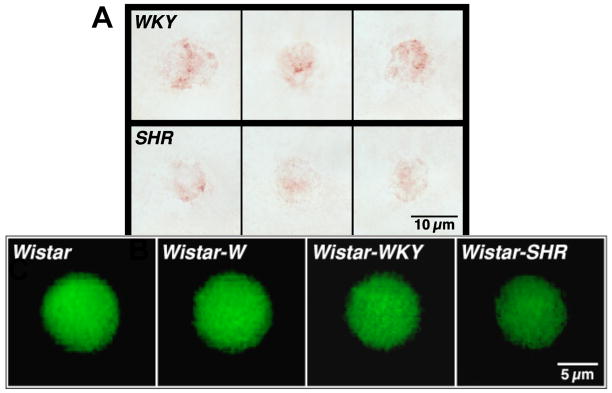
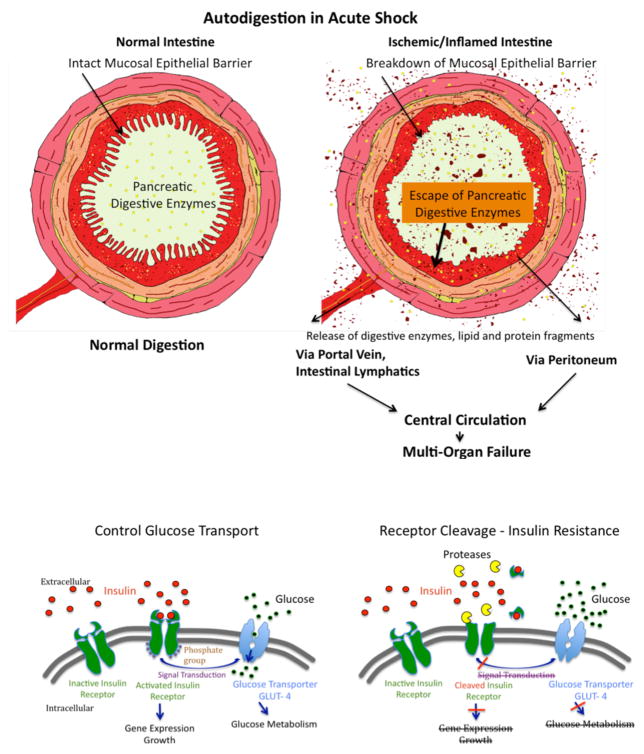
Although long recognized in microvascular research, an increasing body of evidence suggests that inflammatory markers are present in human diseases. Since the inflammatory cascade serves as a repair mechanism, the presence of inflammatory markers in patient groups has raised an important question about the mechanisms that initiate the inflammatory cascade (i.e., the mechanisms that cause tissue injury). Using a severe form of inflammation, shock, and multiorgan failure, for which there is no accepted injury mechanism, we summarize studies that suggest that the powerful pancreatic digestive enzymes play a central role in the destruction of the intestine and other tissues if their compartmentalization in the lumen of the intestine and in the pancreas is compromised. Further, we summarize evidence that uncontrolled degrading enzyme activity in plasma causes proteolytic cleavage of the extracellular domain of membrane receptors and loss of associated cell functions. For example, in a model of metabolic disease with type II diabetes, proteolytic cleavage of the insulin receptor causes the inability of insulin to signal glucose transport across membranes. The evidence suggests that uncontrolled proteolytic and lipolytic enzyme activity may trigger the mechanism for tissue injury. The significance of such mechanisms remain to be explored in human diseases.
Figures
Similar articles
-
The autodigestion hypothesis: Proteolytic receptor cleavage in rheological and cardiovascular cell dysfunction1.Biorheology. 2016;53(5-6):179-191. doi: 10.3233/BIR-17131. Biorheology. 2016. PMID: 28269737 Free PMC article.
-
A new hypothesis for microvascular inflammation in shock and multiorgan failure: self-digestion by pancreatic enzymes.Microcirculation. 2005 Jan-Feb;12(1):71-82. doi: 10.1080/10739680590896009. Microcirculation. 2005. PMID: 15804975 Review.
-
Autodigestion: Proteolytic Degradation and Multiple Organ Failure in Shock.Shock. 2016 May;45(5):483-9. doi: 10.1097/SHK.0000000000000544. Shock. 2016. PMID: 26717111 Free PMC article. Review.
-
A journey with Tony Hugli up the inflammatory cascade towards the auto-digestion hypothesis.Int Immunopharmacol. 2007 Dec 20;7(14):1845-51. doi: 10.1016/j.intimp.2007.07.015. Epub 2007 Aug 9. Int Immunopharmacol. 2007. PMID: 18039521 Free PMC article. Review.
-
Pancreatic digestive enzyme blockade in the small intestine prevents insulin resistance in hemorrhagic shock.Shock. 2014 Jan;41(1):55-61. doi: 10.1097/SHK.0000000000000048. Shock. 2014. PMID: 24088998 Free PMC article.
Cited by
-
Intraluminal nonbacterial intestinal components control gut and lung injury after trauma hemorrhagic shock.Ann Surg. 2014 Dec;260(6):1112-20. doi: 10.1097/SLA.0000000000000631. Ann Surg. 2014. PMID: 24646554 Free PMC article.
-
Hyperthermia induces injury to the intestinal mucosa in the mouse: evidence for an oxidative stress mechanism.Am J Physiol Regul Integr Comp Physiol. 2012 Apr;302(7):R845-53. doi: 10.1152/ajpregu.00595.2011. Epub 2012 Jan 11. Am J Physiol Regul Integr Comp Physiol. 2012. PMID: 22237593 Free PMC article.
-
Pancreatic digestive enzyme blockade in the intestine increases survival after experimental shock.Sci Transl Med. 2013 Jan 23;5(169):169ra11. doi: 10.1126/scitranslmed.3005046. Sci Transl Med. 2013. PMID: 23345609 Free PMC article.
-
Papain Suppresses Atopic Skin Inflammation through Anti-Inflammatory Activities Using In Vitro and In Vivo Models.Antioxidants (Basel). 2024 Jul 30;13(8):928. doi: 10.3390/antiox13080928. Antioxidants (Basel). 2024. PMID: 39199175 Free PMC article.
-
Investigating the Relationship between Epigenetic Age and Cardiovascular Risk in a Population with Overweight/Obesity.Biomedicines. 2024 Jul 23;12(8):1631. doi: 10.3390/biomedicines12081631. Biomedicines. 2024. PMID: 39200095 Free PMC article.
References
-
- Abraham CR, Potter H. The protease inhibitor, alpha 1-antichymotrypsin, is a component of the brain amyloid deposits in normal aging and Alzheimer’s disease. Ann Med. 1989;21:77–81. - PubMed
-
- Acosta JA, Hoyt DB, Schmid-Schönbein GW, Hugli TE, Anjaria DJ, Frankel DA, Coimbra R. Intraluminal pancreatic serine protease activity, mucosal permeability, and shock: a review. Shock. 2006;26:3–9. - PubMed
-
- Adams CA, Jr, Xu DZ, Lu Q, Deitch EA. Factors larger than 100 kd in post-hemorrhagic shock mesenteric lymph are toxic for endothelial cells. Surgery. 2001;129:351–63. - PubMed
-
- Ahmad E, Steinberg SM, Goldin L, Hess CJ, Caporaso N, Kreitman RJ, Wiestner A, Wilson W, White T, Marti G, Stetler-Stevenson M. Immunophenotypic features distinguishing familial chronic lymphocytic leukemia from sporadic chronic lymphocytic leukemia. Cytometry B Clin Cytom. 2008;74:221–6. - PubMed
-
- Arndt H, Smith CW, Granger DN. Leukocyte-endothelial cell adhesion in spontaneously hypertensive and normotensive rats. Hypertension. 1993;21:667–73. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
