

Validation study of an automated electronic acute lung injury screening tool
- PMID: 19390095
- PMCID: PMC2705253
- DOI: 10.1197/jamia.M3120
Validation study of an automated electronic acute lung injury screening tool
Abstract
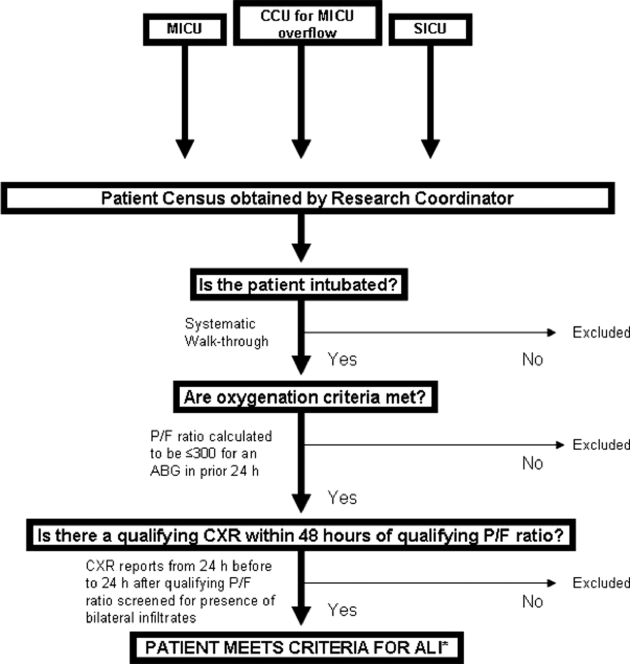
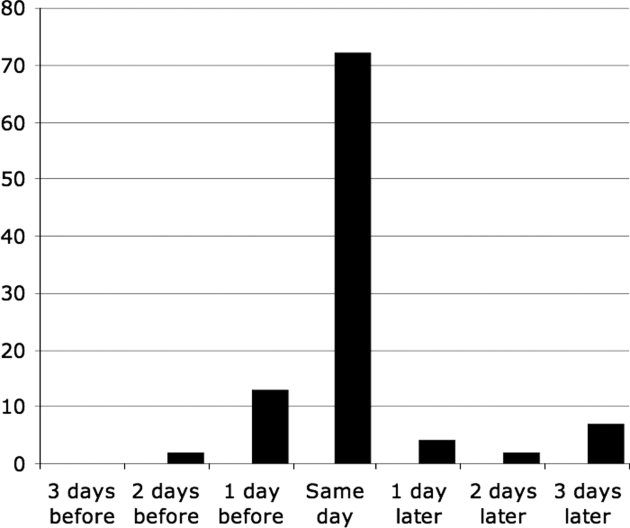
OBJECTIVE The authors designed an automated electronic system that incorporates data from multiple hospital information systems to screen for acute lung injury (ALI) in mechanically ventilated patients. The authors evaluated the accuracy of this system in diagnosing ALI in a cohort of patients with major trauma, but excluding patients with congestive heart failure (CHF). DESIGN Single-center validation study. Arterial blood gas (ABG) data and chest radiograph (CXR) reports for a cohort of intensive care unit (ICU) patients with major trauma but excluding patients with CHF were screened prospectively for ALI requiring intubation by an automated electronic system. The system was compared to a reference standard established through consensus of two blinded physician reviewers who independently screened the same population for ALI using all available ABG data and CXR images. The system's performance was evaluated (1) by measuring the sensitivity and overall accuracy, and (2) by measuring concordance with respect to the date of ALI identification (vs. reference standard). MEASUREMENTS One hundred ninety-nine trauma patients admitted to our level 1 trauma center with an initial injury severity score (ISS) >/= 16 were evaluated for development of ALI in the first five days in an ICU after trauma. Main RESULTS The system demonstrated 87% sensitivity (95% confidence interval [CI] 82.3-91.7) and 89% specificity (95% CI 84.7-93.4). It identified ALI before or within the 24-hour period during which ALI was identified by the two reviewers in 87% of cases. CONCLUSIONS An automated electronic system that screens intubated ICU trauma patients, excluding patients with CHF, for ALI based on CXR reports and results of ABGs is sufficiently accurate to identify many early cases of ALI.
Figures
References
-
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. Am J Respir Crit Care Med 1994;149(3 Pt 1):818-824Mar. - PubMed
-
- Rubenfeld GD, Caldwell E, Peabody E, et al. Incidence and outcomes of acute lung injury N Engl J Med 2005;353(16):1685-1693Oct 20. - PubMed
-
- Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilation strategy on mortality in the acute respiratory distress syndrome N Engl J Med 1998;338(6):347-354Febr 5. - PubMed
-
- The Acute Respiratory Distress Syndrome Network Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome N Engl J Med 2000;342(18):1301-1308May 4. - PubMed
-
- Kalhan R, Mikkelsen M, Dedhiya P, et al. Underuse of lung protective ventilation: Analysis of potential factors to explain physician behavior Crit Care Med 2006;34(2):300-306Febr. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
