

Anti-EGFR Therapy: Mechanism and Advances in Clinical Efficacy in Breast Cancer
- PMID: 19390622
- PMCID: PMC2668926
- DOI: 10.1155/2009/526963
Anti-EGFR Therapy: Mechanism and Advances in Clinical Efficacy in Breast Cancer
Abstract
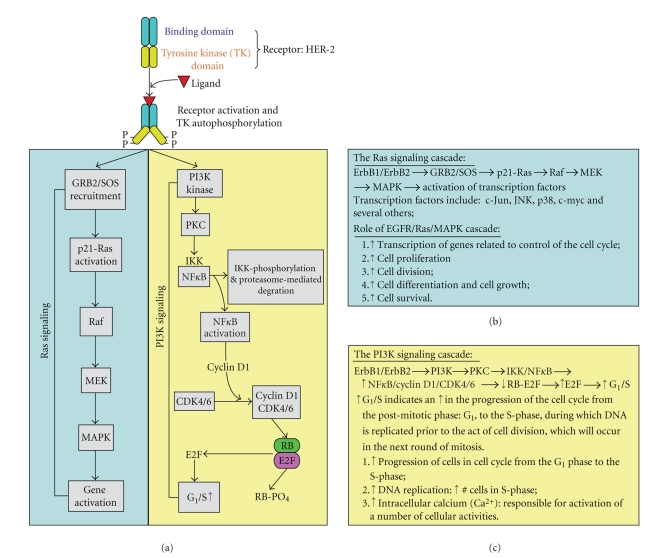
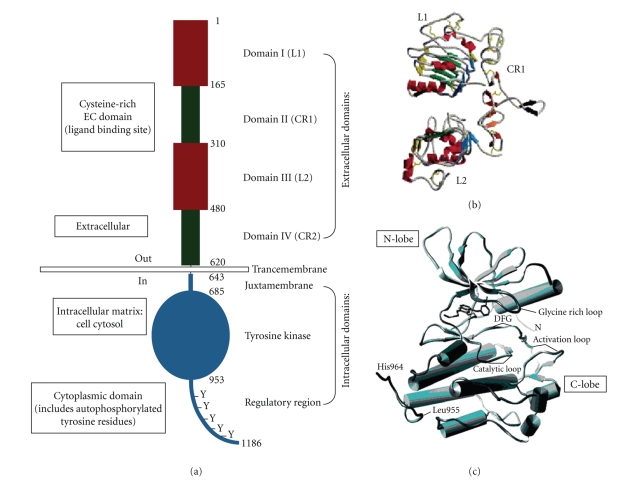
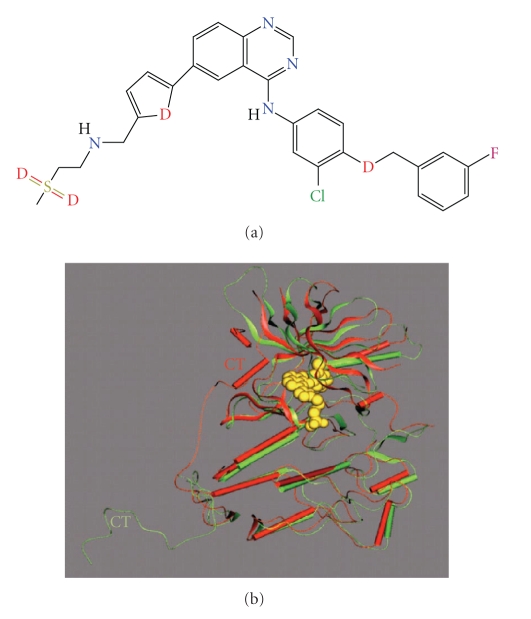
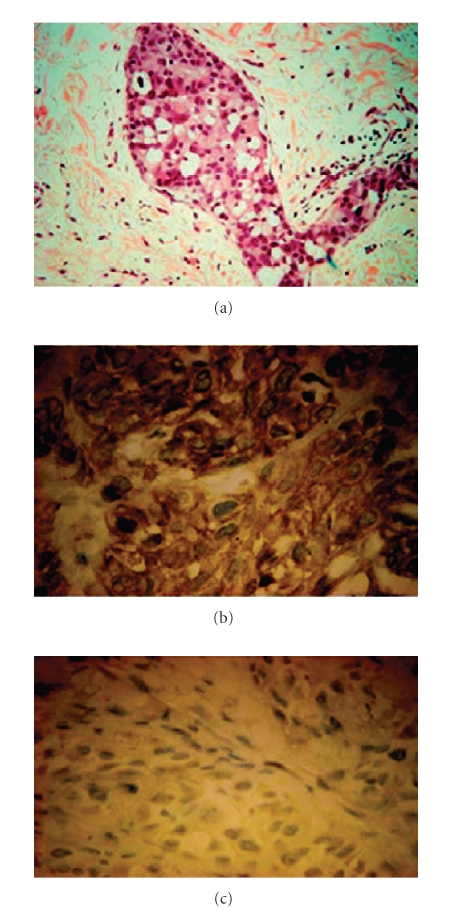
This review will focus on recent advances in the application of antiepidermal growth factor receptor (anti-EGFR) for the treatment of breast cancer. The choice of EGFR, a member of the ErbB tyrosine kinase receptor family, stems from evidence pinpointing its role in various anti-EGFR therapies. Therefore, an increase in our understanding of EGFR mechanism and signaling might reveal novel targets amenable to intervention in the clinic. This knowledge base might also improve existing medical treatment options and identify research gaps in the design of new therapeutic agents. While the approved use of drugs like the dual kinase inhibitor Lapatinib represents significant advances in the clinical management of breast cancer, confirmatory studies must be considered to foster the use of anti-EGFR therapies including safety, pharmacokinetics, and clinical efficacy.
Figures
References
-
- Moy B, Goss PE. Lapatinib: current status and future directions in breast cancer. Oncologist. 2006;11(10):1047–1057. - PubMed
-
- Boyd MC. A Literature Review Submitted to the Program for Biochemistry and Molecular Biology at New York Medical College in Partial Fulfillment of the Requirements for the Degree of Master of Science. Valhalla, NY, USA: Laboratory of Dr. Joseph Wu, New York Medical College; 2005. Epidermal growth factor receptor: structural basis for functional properties.
-
- Gotoh N, Tojo A, Hino M, Yazaki Y, Shibuya M. A highly conserved tyrosine residue at codon 845 within the kinase domain is not required for the transforming activity of human epidermal growth factor receptor. Biochemical and Biophysical Research Communications. 1992;186(2):768–774. - PubMed
-
- Konecny GE, Pegram MD, Venkatesan N, et al. Activity of the dual kinase inhibitor lapatinib (GW572016) against HER-2-overexpressing and trastuzumab-treated breast cancer cells. Cancer Research. 2006;66(3):1630–1639. - PubMed
-
- Agrawal A, Gutteridge E, Gee JMW, Nicholson RI, Robertson JFR. Overview of tyrosine kinase inhibitors in clinical breast cancer. Endocrine-Related Cancer. 2005;12(supplement 1):S135–S144. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
