

Optimal dosing and dynamic distribution of vaccines in an influenza pandemic
- PMID: 19395691
- PMCID: PMC2691801
- DOI: 10.1093/aje/kwp072
Optimal dosing and dynamic distribution of vaccines in an influenza pandemic
Abstract
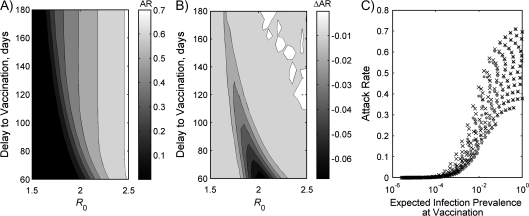
Limited production capacity and delays inherent in vaccine development are major hurdles to the widespread use of vaccines to mitigate the effects of a new influenza pandemic. Antigen-sparing vaccines have the most potential to increase population coverage but may be less efficacious. The authors explored this trade-off by applying simple models of influenza transmission and dose response to recent clinical trial data. In this paper, these data are used to illustrate an approach to comparing vaccines on the basis of antigen supply and inferred efficacy. The effects of delays in matched vaccine availability and seroconversion on epidemic size during pandemic phase 6 were also studied. The authors infer from trial data that population benefits stem from the use of low-antigen vaccines. Delayed availability of a matched vaccine could be partially alleviated by using a 1-dose vaccination program with increased coverage and reduced time to full protection. Although less immunogenic, an overall attack rate of up to 6% lower than a 2-dose program could be achieved. However, if prevalence at vaccination is above 1%, effectiveness is much reduced, emphasizing the need for other control measures.
Figures


References
-
- Fedson DS. Pandemic influenza and the global vaccine supply. Clin Infect Dis. 2003;36(12):1552–1561. - PubMed
-
- Daems R, Del Giudice G, Rappuoli R. Anticipating crisis: towards a pandemic flu vaccination strategy through alignment of public health and industrial policy. Vaccine. 2005;23(50):5732–5742. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
