

Anti-malarial prescriptions in three health care facilities after the emergence of chloroquine resistance in Niakhar, Senegal (1992-2004)
- PMID: 19397797
- PMCID: PMC2680903
- DOI: 10.1186/1475-2875-8-83
Anti-malarial prescriptions in three health care facilities after the emergence of chloroquine resistance in Niakhar, Senegal (1992-2004)
Abstract
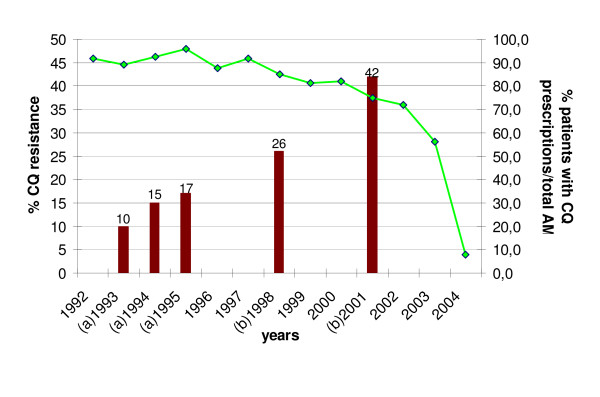
Background: In the rural zone of Niakhar in Senegal, the first therapeutic failures for chloroquine (CQ) were observed in 1992. In 2003, the national policy regarding first-line treatment of uncomplicated malaria was modified, replacing CQ by a transitory bi-therapy amodiaquine/sulphadoxine-pyrimethamine (AQ/SP), before the implementation of artemisinin-based combination therapy (ACT) in 2006. The aims of the study were to assess the evolution of anti-malarial prescriptions in three health care facilities between 1992 and 2004, in parallel with increasing CQ resistance in the region.
Methods: The study was conducted in the area of Niakhar, a demographic surveillance site located in a sahelo-sudanese region of Senegal, with mesoendemic and seasonal malaria transmission. Health records of two public health centres and a private catholic dispensary were collected retrospectively to cover the period 1992-2004.
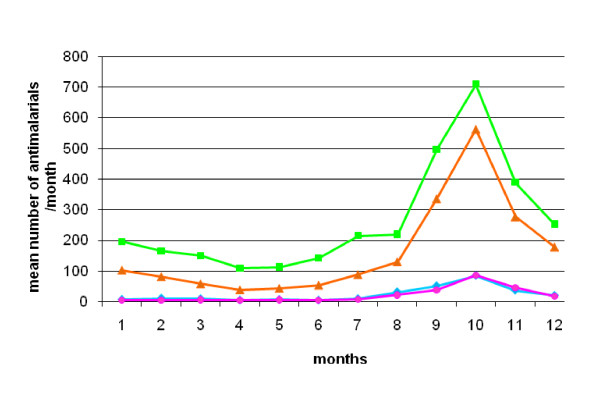
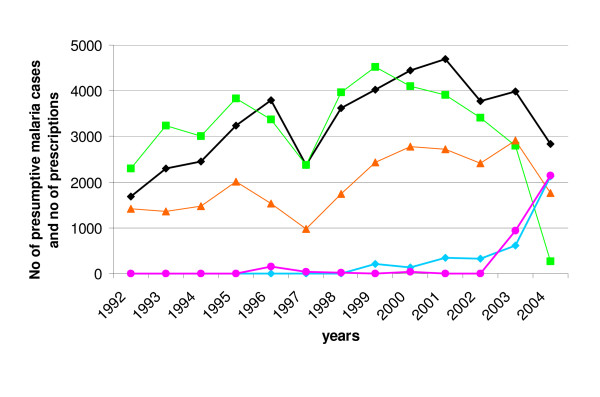
Results: Records included 110,093 consultations and 292,965 prescribed treatments. Twenty-five percent of treatments were anti-malarials, prescribed to 49% of patients. They were delivered all year long, but especially during the rainy season, and 20% of patients with no clinical malaria diagnosis received anti-malarials. Chloroquine and quinine represented respectively 55.7% and 34.6% of prescribed anti-malarials. Overall, chloroquine prescriptions rose from 1992 to 2000, in parallel with clinical malaria; then the CQ prescription rate decreased from 2000 and was concomitant with the rise of SP and the persistence of quinine use. AQ and SP were mainly used as bi-therapy after 2003, at the time of national treatment policy change.
Conclusion: The results show the overall level of anti-malarial prescription in the study area for a considerable number of patients over a large period of time. Even though resistance to CQ rapidly increased from 1992 to 2001, no change in CQ prescription was observed until the early 2000s, possibly due to the absence of an obvious decrease in CQ effectiveness, a lack of therapeutic options or a blind follow-up of national guidelines.
Figures
References
-
- Young MD, Moore DV. Chloroquine resistance in Plasmodium falciparum. Am J Trop Med Hyg. 1961;10:317–320. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
