

doi: 10.1136/jcp.2008.059782.
My approach to interstitial lung disease using clinical, radiological and histopathological patterns
Affiliations
- PMID: 19398592
- PMCID: PMC2668105
- DOI: 10.1136/jcp.2008.059782
Item in Clipboard
My approach to interstitial lung disease using clinical, radiological and histopathological patterns
J Clin Pathol.
2009 May.
Abstract
The complex world of interstitial lung disease presents nearly insurmountable challenges to the general surgical pathologist faced with a lung biopsy in this setting. The pathology is often inflammatory and always requires clinical and radiological context for a relevant and clinically useful histopathological diagnosis. A pattern-based histopathological approach to interstitial lung disease provides a "map" for the general pathologist to navigate this area successfully, especially so when used with aid of the clinical and radiological patterns of presentation.
Conflict of interest statement
Figures

Pattern 1: acute lung injury. At scanning magnification (2× objective), the biopsy sections have an eosinophilic appearance. H&E stain, 15× original magnification.

Diffuse alveolar damage. (A) Alveoli are empty and lined by hyaline membranes or (B) variably filled by oedema, macrophages and immature fibroblasts (organisation; OP). Residual hyaline membranes are often present (arrow). H&E stain, 100× original magnification.

Acute injury with necrosis. Necrosis (N) is a harbinger of infection in the context of pattern 1 and an acutely ill patient. Infection always leads the differential diagnosis in this situation, even if special stains are negative. H&E stain, 100× original magnification.

Acute eosinophilic pneumonia. (A) When many eosinophils are visible in the airspaces in a patient with acute lung disease, a diagnosis of acute eosinophilic pneumonia is appropriate. (B) Organisation in alveolar spaces, and rarely hyaline membranes, may be present. (A,B) H&E stain, 100× original magnification.

Diffuse alveolar haemorrhage. (A) The lung biopsy specimen has variable fresh blood in the parenchyma, typically associated with fibrin, reactive type 2 cells and haemosiderin-filled alveolar macrophages (B). This reaction pattern may be associated with immunologically mediated injury. (A,B) H&E stain; (A) 40× original magnification; (B) 400× original magnification.

Capillaritis in diffuse alveolar haemorrhage. (A) The presence of capillaritis is one of the few medical emergencies in pulmonary pathology. Capillaritis is distinctive but can be quite focal in the biopsy specimen. Here a “pseudo-bronchopneumonia” pattern is present, with shed neutrophils filling alveolar spaces. (B) Here the neutrophils are still within the alveolar walls. (A,B) H&E stain; (A) 40× original magnification; (B) 400× original magnification.

Pattern 2 fibrosis. Fibrosis in the lung parenchyma should be diagnosed only when it is dense, and never in the transbronchial biopsy specimen. Note the distortion of the alveolar parenchyma and fusion of alveolar walls.

Honeycomb remodelling. (A) Large, often stacked, cystic spaces seen in whole-lung sections are referred to as “honeycomb cysts”. (B) These are often recapitulated (or preceded) at the microscopic level, where the process is referred to as “microscopic honeycombing”. (A) Gross image; (B) H&E stain, 1× original magnification.

Usual interstitial pneumonia (UIP). UIP is characterised by zones of normal lung tissue adjacent to zones of advanced architectural remodelling (temporal heterogeneity). (A) Early in the disease process, an interrupted “rind” of subpleural fibrosis is visible. (B) A more advanced stage shows more extensive perilobular fibrosis with relative centrilobular sparing, producing ring-like scarring at scanning magnification. (A,B) H&E stain, 1× original magnification.

Microscopic honeycombing. This finding occurs early in usual interstitial pneumonia and consists of irregular microscopic cysts containing mucus (with neutrophils) and lined by ciliated columnar epithelium. H&E stain, 40× original magnification.

Fibroblast foci. Discrete “bulges” of immature fibroblasts in amphophilic matrix are referred to as “fibroblast” or “fibroblastic” foci. They occur at the interface between dense scar and adjacent normal lung. In a three-dimensional reconstruction study, the foci appear to be interconnected into a lattice. These lesions are thought to be the focus of ongoing injury and repair in usual interstitial pneumonia (UIP), but are not unique to UIP. H&E stain, 200× original magnification.

Diffuse alveolar wall fibrosis. Sometimes “interstitial” fibrosis preserves alveolar structure (ie, little confluence of scar) invoking a fairly limited differential diagnosis, dominated by rheumatic diseases, chronic drug reactions and some examples of chronic hypersensitivity. When no underlying aetiology is present, the term “idiopathic NSIP” is appropriate. H&E stain, 40× original magnification.

Airway-centred fibrosis. Fibrosis around bronchioles is typically a manifestation of inhalational or aspiration injury to the lungs. H&E stain, 15× original magnification.

Langerhans cell histiocytosis (LCH). The star-shaped, airway-centred scars of LCH are distinctive and may be a sign of resolved disease. H&E stain, 15× original magnification.

Pattern 3: chronic inflammatory (cellular) infiltrates. The biopsy specimen in pattern 3 tends to have a blue appearance because of the interstitial infiltrates of mononuclear cells (mainly lymphocytes and plasma cells) with their haematoxylin-stained nuclei and scant cytoplasm. H&E stain, 15× original magnification.

Non-specific interstitial pneumonia (NSIP), cellular. The pure cellular form of NSIP is rare. If small poorly formed granulomas are present, hypersensitivity pneumonitis should be considered. If foci of organising pneumonia are present, without granulomas, cryptogenic organising pneumonia should be considered. H&E stain, 40× original magnification.

Hypersensitivity pneumonitis (HP). The cellular interstitium of subacute HP (A) is dominated by plasma cells (magnification in B). A typical poorly formed granuloma of HP is present in (B). (A,B) H&E stain; (A) 40× original magnification; (B) 400× original magnification.

Granulomatous pneumonia from infection. This example of atypical mycobacterial infection (Mycobacterium avium complex) differs from hypersensitivity pneumonitis in having larger and better formed granulomas, along with more granulomas in the alveolar spaces and alveolar ducts. Necrosis in granulomas may be present (not in this image) and is a harbinger of infection. Sarcoidosis granulomas (fig 25) are better formed, have less associate inflammation, and consistently have more hyaline fibrosis around aggregated granulomas. H&E stain, 40× original magnification.

Pattern 4: alveolar filling. This example of diffuse alveolar haemorrhage nicely demonstrates the concept of alveolar filling. In cases of inflammatory reaction to injury, initial interstitial changes typically evolve to alveolar filling disease (eg, acute bronchopneumonia, organising pneumonia). H&E stain, 15× original magnification.

Cryptogenic organising pneumonia (COP). The most consistent finding in COP is patchy involvement of the airspaces by small tufts of immature fibroblasts distributed within terminal bronchioles, alveolar ducts and alveoli. H&E stain, 40× original magnification.

Desquamative interstitial pneumonia (DIP). Idiopathic DIP is characterised by dense alveolar macrophages. Many conditions can result in localised alveolar macrophage accumulation. Inset: alveolar macrophage detail. H&E stain, 40× original magnification (inset, 400× original magnification).

Exogenous lipoid pneumonia. The microscopic appearance of exogenous lipoid pneumonia is dependent on the composition of the aspirated material. (A) Exogenous lipoid pneumonia with histiocytes containing predominantly fine microvesicles. (B) Exogenous lipoid pneumonia with larger vacuoles and associated fibrosis. (A,B) H&E stain, 40× original magnification.

Pulmonary alveolar proteinosis (PAP). All of the diagnostic features of PAP are identifiable in this image: alveolar exudates with an eosinophilic granular appearance, scattered larger inclusions with more intense eosin staining, and slight retraction effect at the periphery of the alveolus. H&E stain, 40× original magnification.

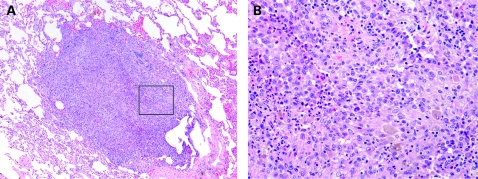
Pattern 5: nodules. In pattern 5, nodules may be well or poorly formed, large or small, single or numerous. This is a patient with sarcoidosis. H&E stain, 15× original magnification.

Sarcoidosis. Sarcoid granulomas surrounded by dense, brightly eosinophilic lamellar collagen. Note the rosette-like adventitial distribution in this example. The central structure in this image is a pulmonary artery. H&E stain, 40× original magnification.

Silicatosis. Similar to sarcoidosis in distribution, the nodules of silicate disease can be distinguished by the common occurrence of dark pigment dust and the characteristic fibroblastic proliferation that occurs in response to silicate dust. When these morphological features are present, refractile silicate particles that rotate plane-polarised light are always present. This was a patient with mixed dust pneumoconiosis. H&E stain, 40× original magnification.
Langerhans cell histiocytosis (LCH). LCH has variable morphology. The cellular form can suggest neoplasm (A). At higher magnification, the characteristic admixture of pale amphophilic Langerhans cells, lightly pigmented macrophages and eosinophils confirms the diagnosis (B). (A,B) H&E stain; (A) 40× original magnification; (B) 400× original magnification.

Pattern 6: minimal changes. Pattern 6 is defined by little evident pathology at scanning magnification. This patient has constrictive bronchiolitis and was severely hypoxic. There should be a bronchiole for nearly every pulmonary artery in this field (and the pair should be of nearly equal diameter in cross-section). H&E stain, 15× original magnification.

Constrictive bronchiolitis. The injury in constrictive bronchiolitis is often multifocal, resulting in varicosity of the terminal airways. Here a small scarred bronchiole is present next to two profiles of a recently bifurcated pulmonary artery. H&E stain, 40× original magnification.
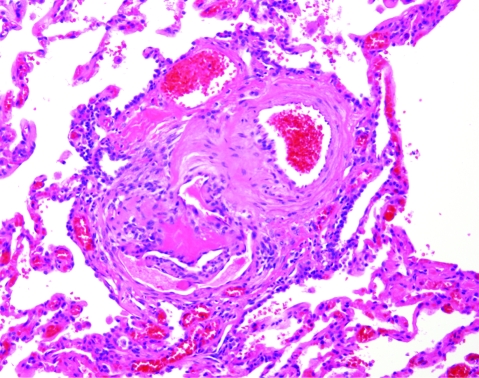
Plexiform lesion of pulmonary hypertension. This classical plexiform lesion is composed of a pulmonary artery profile (upper right of centre) with an adjacent glomeruloid structure (lower left of centre). An early dilatation lesion is also present here (thin-walled, dilated vessels at the edges of the complex). H&E stain, 40× original magnification.
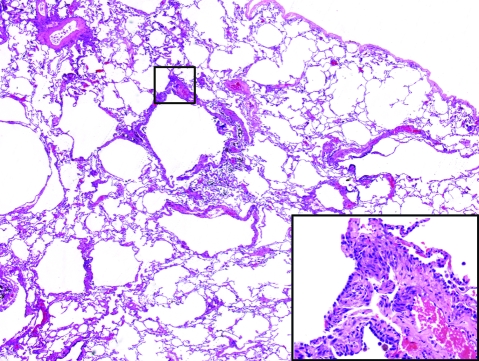
Lymphangioleiomyomatosis. The cysts of lymphangioleiomyomatosis can be quite subtle in surgical lung biopsy samples. Once a cyst is identified, a search for thickened cellular areas of the wall will reveal the aggregated fascicles of hyperchromatic and slightly disorganised smooth muscle of lymphangioleiomyomatosis (inset). H&E stain, 15× original magnification; inset: 400× original magnification.
References
-
- Leslie K, Colby T, Swenson S. Anatomic distribution and histopathologic patterns of interstitial lung disease. Schwartz M I, King T E, eds. Interstitial lung disease Hamilton: BC Decker, 2003
-
- Leslie K, Wick M. Practical pulmonary pathology. A diagnostic approach Philadelphia: Churchill-Livingstone, 2005
-
- Leslie KO. Pulmonary pathology for the clinician. Clin Chest Med. 2006;27:S1–10, v. - PubMed
-
- Leslie KO, Gruden JF, Parish JM, et al. Transbronchial biopsy interpretation in the patient with diffuse parenchymal lung disease. Arch Pathol Lab Med 2007;131:407–23 - PubMed
-
- Elicker B, Pereira CA, Webb R, et al. High-resolution computed tomography patterns of diffuse interstitial lung disease with clinical and pathological correlation. J Bras Pneumol 2008;34:715–44 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical