

Risk of dementia in MCI: combined effect of cerebrovascular disease, volumetric MRI, and 1H MRS
- PMID: 19398707
- PMCID: PMC2843530
- DOI: 10.1212/WNL.0b013e3181a2e864
Risk of dementia in MCI: combined effect of cerebrovascular disease, volumetric MRI, and 1H MRS
Abstract
Objective: To investigate the combined ability of hippocampal volumes, 1H magnetic resonance spectroscopy (MRS) metabolites, and cerebrovascular disease to predict the risk of progression to dementia in mild cognitive impairment (MCI).
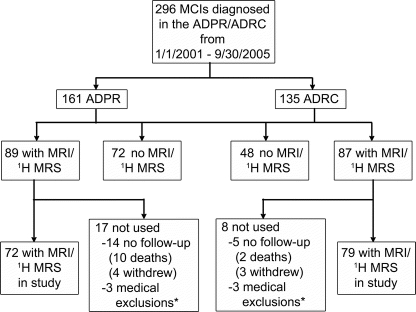
Methods: We identified 151 consecutively recruited subjects with MCI from the Mayo Clinic Alzheimer's Disease Research Center and Patient Registry who underwent MRI and 1H MRS studies at baseline and were followed up with approximately annual clinical examinations. A multivariable proportional hazards model that considered all imaging predictors simultaneously was used to determine whether hippocampal volumes, posterior cingulate gyrus 1H MRS metabolites, white matter hyperintensity load, and presence of cortical and subcortical infarctions are complementary in predicting the risk of progression from MCI to dementia.
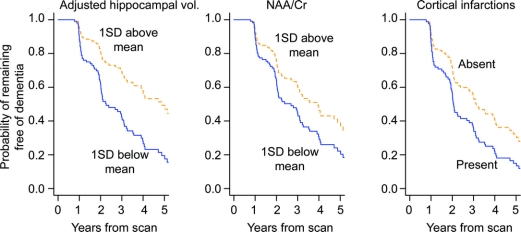
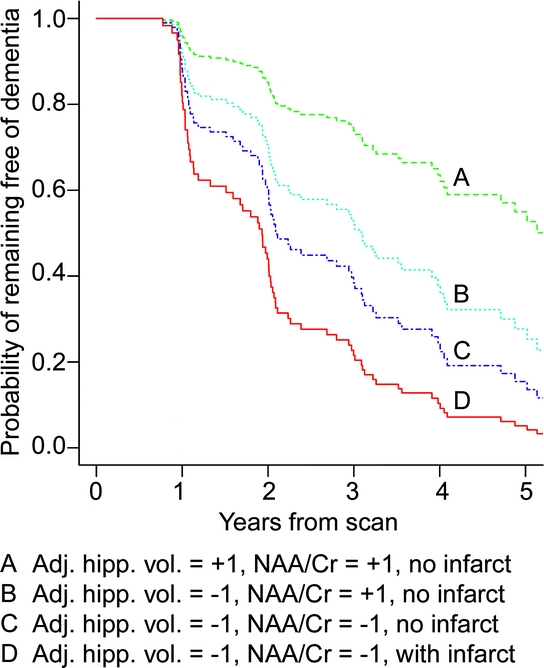
Results: Seventy-five subjects with MCI progressed to dementia by last follow-up. The model that best predicted progression to dementia included age, sex, hippocampal volumes, N-acetylaspartate (NAA)/creatine (Cr) on 1H MRS, and cortical infarctions. Based on age- and sex-adjusted Kaplan-Meier plots, we estimated that by 3 years, 26% of the MCI patients with normal hippocampal volumes, NAA/Cr ratios >1 SD, and no cortical infarctions will progress to dementia, compared with 78% of the MCI patients with hippocampal atrophy, low NAA/Cr (< or =1 SD), and cortical infarction.
Conclusions: Multiple magnetic resonance (MR) markers of underlying dementia pathologies improve the ability to identify patients with prodromal dementia over a single MR marker, supporting the concept that individuals with multiple brain pathologies have increased odds of dementia compared with individuals with a single pathology.
Figures
References
-
- Petersen RC, Stevens JC, Ganguli M, Tangalos EG, Cummings JL, DeKosky ST. Practice parameter: early detection of dementia—mild cognitive impairment (an evidence-based review). Report of the Quality Standards Subcommittee of the American Academy of Neurology. Neurology 2001;56:1133–1142. - PubMed
-
- Morris JC, Storandt M, Miller JP, et al. Mild cognitive impairment represents early-stage Alzheimer disease. Arch Neurol 2001;58:397–405. - PubMed
-
- Busse A, Hensel A, Guhne U, Angermeyer MC, Riedel-Heller SG. Mild cognitive impairment: long-term course of four clinical subtypes. Neurology 2006;67:2176–2185. - PubMed
-
- Di Carlo A, Lamassa M, Baldereschi M, et al. CIND and MCI in the Italian elderly: frequency, vascular risk factors, progression to dementia. Neurology 2007;68:1909–1916. - PubMed
-
- Fischer P, Jungwirth S, Zehetmayer S, et al. Conversion from subtypes of mild cognitive impairment to Alzheimer dementia. Neurology 2007;68:288–291. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical