

Vacuum-assisted vaginal delivery
Abstract
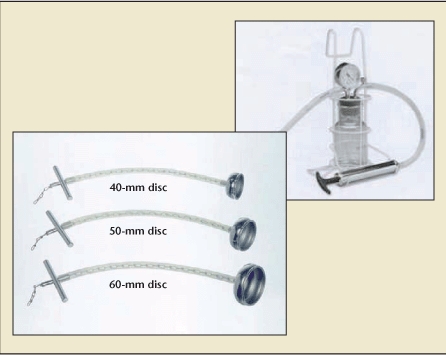
Approximately 5% (1 in 20) of all deliveries in the United States are operative vaginal deliveries. The past 20 years have seen a progressive shift away from the use of forceps in favor of the vacuum extractor as the instrument of choice. This article reviews in detail the indications, contraindications, patient selection criteria, choice of instrument, and technique for vacuum-assisted vaginal delivery. The use of vacuum extraction at the time of cesarean delivery will also be discussed. With vacuum extraction becoming increasingly popular, it is important that obstetric care providers are aware of the maternal and neonatal risks associated with such deliveries and of the options available to effect a safe and expedient delivery.
Keywords: Operative vaginal delivery; Vacuum; Vacuum-assisted vaginal delivery.
Figures


References
-
- Martin JA, Hamilton EB, Sutton PD, et al. Centers for Disease Control and Prevention National Center for Health Statistics National Vital Statistics System. Births: final data for 2002. Natl Vital Stat Rep. 2007;56:1–103. - PubMed
-
- Clark SL, Belfort MA, Hankins GD, et al. Variation in the rates of operative delivery in the United States. Am J Obstet Gynecol. 2007;196:526.e1–526.e5. - PubMed
-
- Kozak LJ, Weeks JD. Trends in obstetric procedures, 1990–2000. Birth. 2002;29:157–161. - PubMed
-
- The American College of Obstetricians and Gynecologists (ACOG), authors Operative Vaginal Delivery. Washington, DC: ACOG; 2000. (Practice Bulletin No. 17).
-
- Malmström T. The vacuum extractor: an obstetrical instrument. Acta Obstet Gynecol Scand. 1957;36:5–50. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous