

Novel concepts in the evaluation and treatment of high-dysplastic spondylolisthesis
- PMID: 19399535
- PMCID: PMC2899600
- DOI: 10.1007/s00586-009-0984-y
Novel concepts in the evaluation and treatment of high-dysplastic spondylolisthesis
Abstract
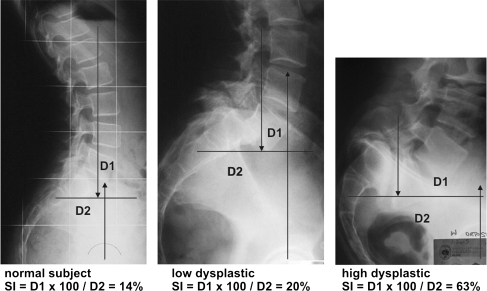
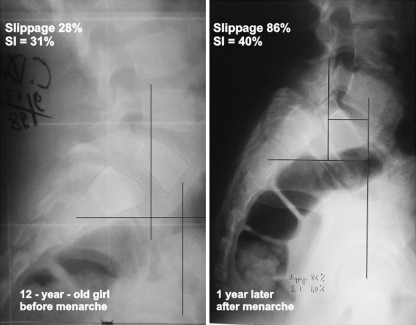
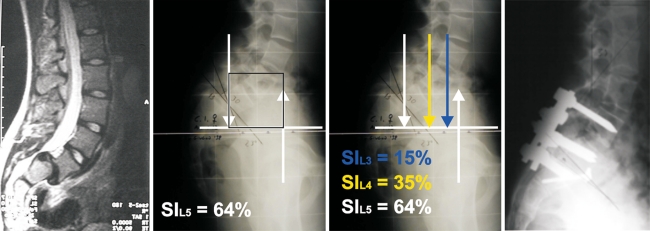
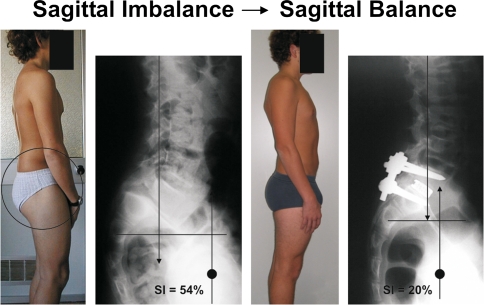
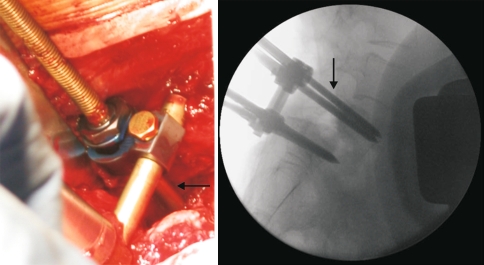
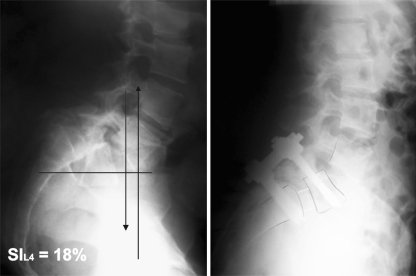
The classification system of spondylolisthesis proposed by Marchetti and Bartolozzi is the most practical regarding prognosis and treatment and includes the description of both low- and high-dysplastic developmental spondylolisthesis (HDDS). Unfortunately, it does not provide strict criteria on how to differentiate between these two subtypes. The accepted treatment for HDDS is surgical. However, there is no consensus on how to surgically stabilize this subtype of spondylolisthesis, and although the concept of reducing spinal deformity before fusion is attractive, the issue of surgical reduction versus in situ fusion remains controversial, especially for HDDS (Meyerding Grades III and IV). The purpose of this study was (1) to describe the severity index (SI) as a simple method that can be used in the identification of low-dysplastic developmental spondylolisthesis from HDDS allowing earlier surgical stabilization to prevent slip progression, (2) to provide guidelines for using the unstable zone for the inclusion of L4 in stabilization, and (3) to describe a surgical technique in the reduction and stabilization of this challenging surgical entity in an attempt to decrease the risk of iatrogenic L5 neurologic injury. The concepts of SI and unstable zone in the evaluation and treatment of HDDS are relatively new. In our study, patients with an SI value >20% were classified as having HDDS and surgical stabilization was offered. In addition, all vertebrae that were contained in the defined unstable zone were surgically instrumented and fused with attempts at anatomic reduction. This case series involved the retrospective radiological review of 25 consecutive patients surgically treated for HDDS between April 2000 and September 2004 by two senior surgeons. All 25 patients had a minimum 3-year follow-up. Reduction of slip, lumbosacral kyphosis, sacral inclination, fusion rate, maintenance of reduction, and iatrogenic L5 neurologic injury were evaluated. Twenty-two patients underwent a single-level L5-S1 fusion. Three patients had extension of the L5-S1 fusion to include L4 because it fell into the unstable zone. Slip improved from 67.2 to 13.6%, focal L5-S1 kyphosis improved from +17.5 degrees to -6.4 degrees . There were no pseudoarthroses and all patients had radiographic evidence of solid bony fusion at latest follow-up. To date, there have been no re-operations secondary to progression of deformity or loss of fixation. Two re-operations were performed, one for a superficial wound infection, the other for further laparoscopic decompression for continued L5 nerve root symptoms after the index surgery. One patient developed an iatrogenic L5 radiculopathy with dysaesthesiae 3 days postoperatively which completely resolved over 6 weeks. HDDS is best treated surgically. Early identification and stabilization of this challenging surgical entity could prevent the progression of slip and deformity making the index surgery less technically demanding. Vertebrae that are contained in the unstable zone can be instrumented and stabilized so that progression of the deformity and re-operation might be avoided. The authors suggested surgical technique can provide a way to restore sagittal balance, provide an environment for successful fusion, and decrease the risk of iatrogenic L5 neurologic injury.
Figures

References
-
- Boxall D, Bradford DS, Winter RB, Moe JH. Management of severe spondylolisthesis in children and adolescents. J Bone Joint Surg Am. 1979;61:479–495. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
