

Using molecular similarity to highlight the challenges of routine immunoassay-based drug of abuse/toxicology screening in emergency medicine
- PMID: 19400959
- PMCID: PMC2688477
- DOI: 10.1186/1471-227X-9-5
Using molecular similarity to highlight the challenges of routine immunoassay-based drug of abuse/toxicology screening in emergency medicine
Abstract
Background: Laboratory tests for routine drug of abuse and toxicology (DOA/Tox) screening, often used in emergency medicine, generally utilize antibody-based tests (immunoassays) to detect classes of drugs such as amphetamines, barbiturates, benzodiazepines, opiates, and tricyclic antidepressants, or individual drugs such as cocaine, methadone, and phencyclidine. A key factor in assay sensitivity and specificity is the drugs or drug metabolites that were used as antigenic targets to generate the assay antibodies. All DOA/Tox screening immunoassays can be limited by false positives caused by cross-reactivity from structurally related compounds. For immunoassays targeted at a particular class of drugs, there can also be false negatives if there is failure to detect some drugs or their metabolites within that class.
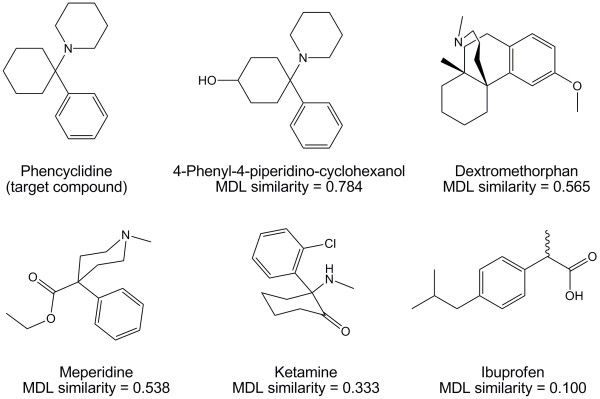
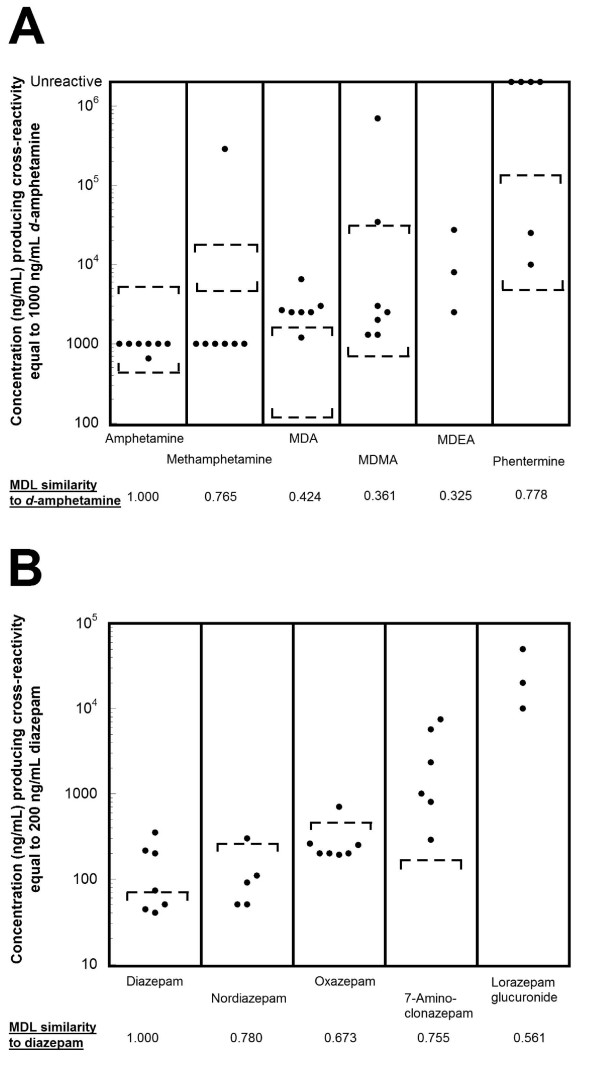
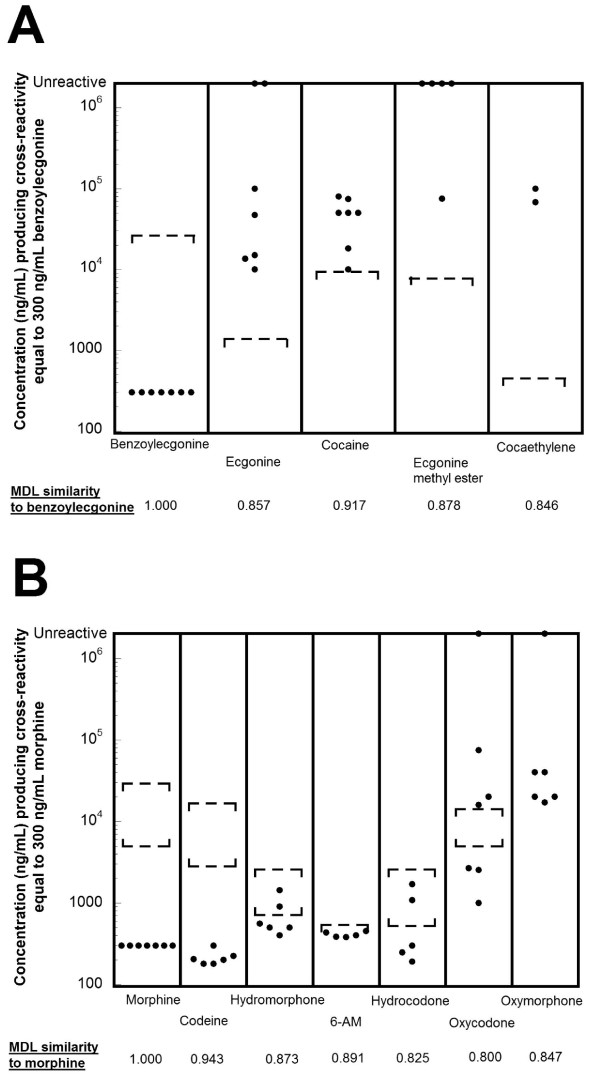
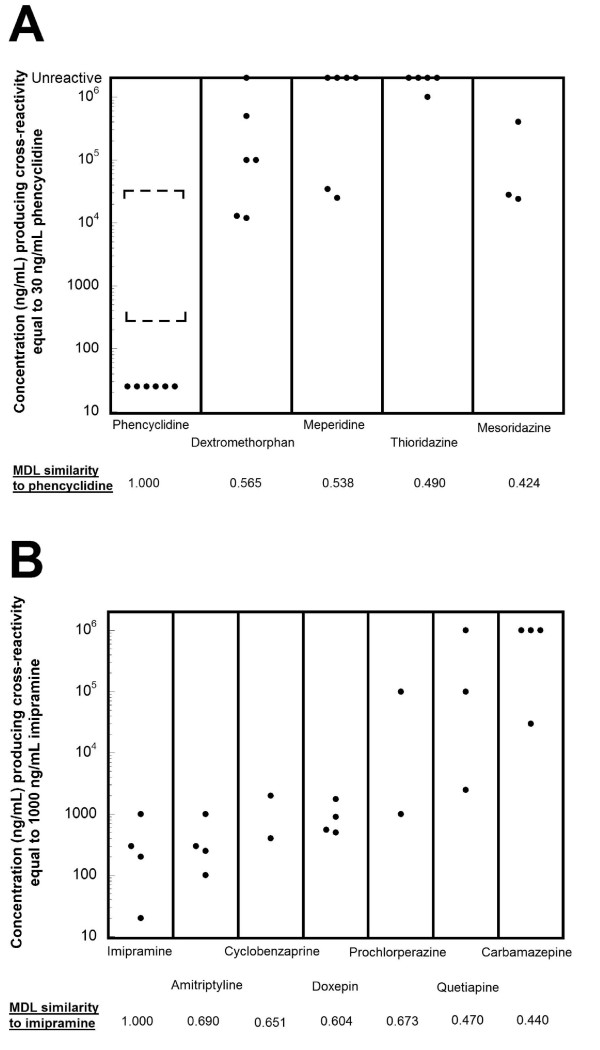
Methods: Molecular similarity analysis, a computational method commonly used in drug discovery, was used to calculate structural similarity of a wide range of clinically relevant compounds (prescription and over-the-counter medications, illicit drugs, and clinically significant metabolites) to the target ('antigenic') molecules of DOA/Tox screening tests. These results were compared with cross-reactivity data in the package inserts of immunoassays marketed for clinical testing. The causes for false positives for phencyclidine and tricyclic antidepressant screening immunoassays were investigated at the authors' medical center using gas chromatography/mass spectrometry as a confirmatory method.
Results: The results illustrate three major challenges for routine DOA/Tox screening immunoassays used in emergency medicine. First, for some classes of drugs, the structural diversity of common drugs within each class has been increasing, thereby making it difficult for a single assay to detect all compounds without compromising specificity. Second, for some screening assays, common 'out-of-class' drugs may be structurally similar to the target compound so that they account for a high frequency of false positives. Illustrating this point, at the authors' medical center, the majority of positive screening results for phencyclidine and tricyclic antidepressants assays were explained by out-of-class drugs. Third, different manufacturers have adopted varying approaches to marketed immunoassays, leading to substantial inter-assay variability.
Conclusion: The expanding structural diversity of drugs presents a difficult challenge for routine DOA/Tox screening that limit the clinical utility of these tests in the emergency medicine setting.
Figures
Similar articles
-
Accidental intoxications in toddlers: lack of cross-reactivity of vilazodone and its urinary metabolite M17 with drug of abuse screening immunoassays.BMC Clin Pathol. 2019 Feb 18;19:2. doi: 10.1186/s12907-019-0084-9. eCollection 2019. BMC Clin Pathol. 2019. PMID: 30820187 Free PMC article.
-
Chemoinformatic methods for predicting interference in drug of abuse/toxicology immunoassays.Clin Chem. 2009 Jun;55(6):1203-13. doi: 10.1373/clinchem.2008.118638. Epub 2009 Apr 2. Clin Chem. 2009. PMID: 19342505 Free PMC article.
-
Lack of Detection of New Amphetamine-Like Drugs Using Conventional Urinary Immunoassays.Ther Drug Monit. 2018 Feb;40(1):135-139. doi: 10.1097/FTD.0000000000000475. Ther Drug Monit. 2018. PMID: 29194289
-
False-positive interferences of common urine drug screen immunoassays: a review.J Anal Toxicol. 2014 Sep;38(7):387-96. doi: 10.1093/jat/bku075. Epub 2014 Jul 1. J Anal Toxicol. 2014. PMID: 24986836 Review.
-
Clinical issues associated with urine testing of substances of abuse.Pharmacotherapy. 1997 May-Jun;17(3):497-510. Pharmacotherapy. 1997. PMID: 9165553 Review.
Cited by
-
Chemiluminescence based immunoassay for the detection of heroin and its metabolites.Bioimpacts. 2018;8(1):53-58. doi: 10.15171/bi.2018.07. Epub 2017 Oct 30. Bioimpacts. 2018. PMID: 29713602 Free PMC article.
-
Point-of-care community drug checking technologies: an insider look at the scientific principles and practical considerations.Harm Reduct J. 2023 Mar 25;20(1):39. doi: 10.1186/s12954-023-00764-3. Harm Reduct J. 2023. PMID: 36966319 Free PMC article. Review.
-
Use of a data warehouse at an academic medical center for clinical pathology quality improvement, education, and research.J Pathol Inform. 2015 Jul 28;6:45. doi: 10.4103/2153-3539.161615. eCollection 2015. J Pathol Inform. 2015. PMID: 26284156 Free PMC article.
-
Phencyclidine false positive induced by lamotrigine (Lamictal®) on a rapid urine toxicology screen.Int J Emerg Med. 2010 Nov 6;3(4):327-31. doi: 10.1007/s12245-010-0235-3. Int J Emerg Med. 2010. PMID: 21373301 Free PMC article.
-
Policy change to improve pathology turnaround time and reduce costs--possible to do both?Biochem Med (Zagreb). 2013;23(3):296-302. doi: 10.11613/bm.2013.035. Biochem Med (Zagreb). 2013. PMID: 24266298 Free PMC article.
References
-
- Wu AHB, McKay C, Broussard LA, Hoffman RS, Kwong TC, Moyer TP, Otten EM, Welch SL, Wax P. National Academy of Clinical Biochemistry laboratory medicine practice guidelines: recommendations for the use of laboratory tests to support poisoned patients who present to the emergency department. Clin Chem. 2003;49:357–379. doi: 10.1373/49.3.357. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
