

Clinical benefit in Phase-I trials of novel molecularly targeted agents: does dose matter?
- PMID: 19401696
- PMCID: PMC2694416
- DOI: 10.1038/sj.bjc.6605030
Clinical benefit in Phase-I trials of novel molecularly targeted agents: does dose matter?
Abstract
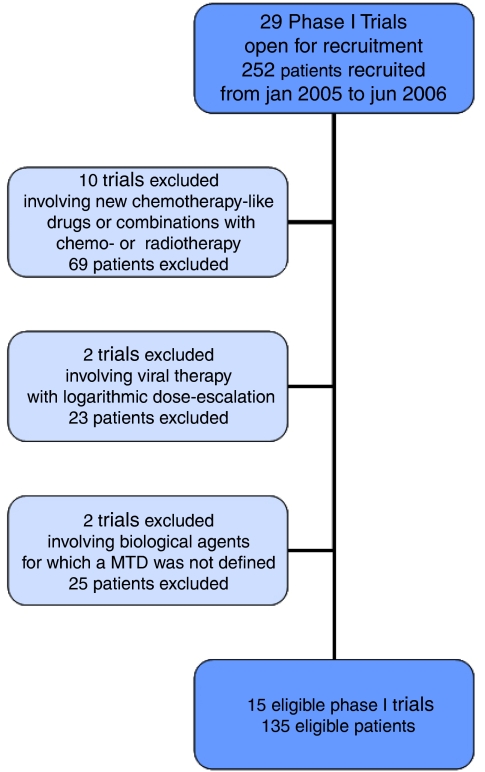
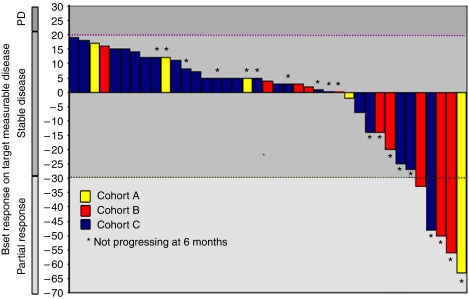
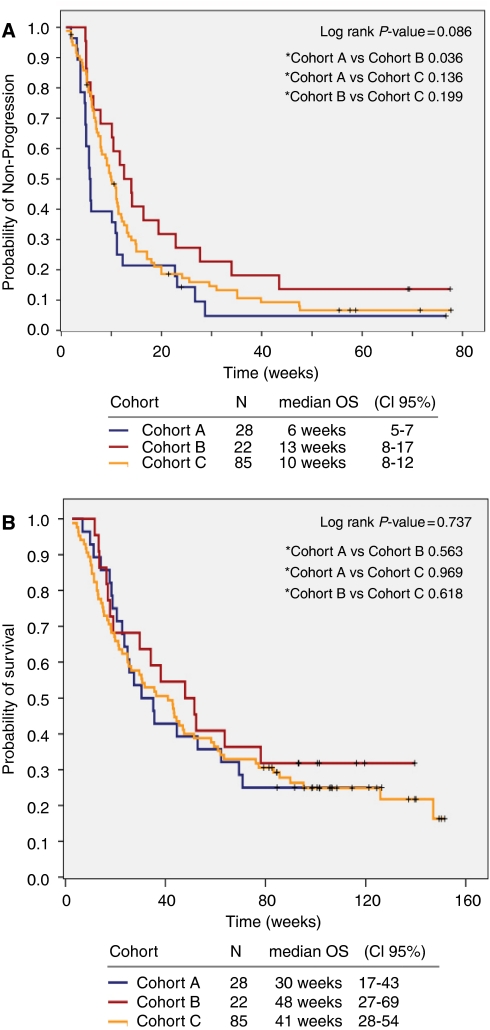
Phase-I trials traditionally involve dose-escalation to determine the maximal tolerated dose (MTD). With conventional chemotherapy, efficacy is generally deemed to be dose-dependent, but the same may not be applicable to molecularly targeted agents (MTAs). We analysed consecutive patients included in Phase-I trials at the Royal Marsden Hospital from 5 January 2005 to 6 June 2006. We considered only trials of monotherapy MTAs in which the MTD was defined. Three patient cohorts (A, B, and C) were identified according to the dose received as a percentage of the final trial MTD (0-33%, 34-65%, >66%). Potential efficacy was assessed using the non-progression rate (NPR), that is, complete/partial response or stable disease for at least 3 months by RECIST. A total of 135 patients having progressive disease before enrolment were analysed from 15 eligible trials. Median age was 57 years (20-86); male : female ratio was 1.8 : 1. Cohort A, B, and C included 28 (21%), 22 (16%), and 85 (63%) patients; NPR at 3 and 6 months was 21% and 11% (A), 50% and 27% (B), 31% and 14% (C), respectively, P=0.9. Median duration of non-progression (17 weeks; 95% CI=13-22) was not correlated with the MTD level, P=0.9. Our analysis suggests that the potential for clinical benefit is not confined to patients treated at doses close to the MTD in Phase-I trials of MTAs.
Figures
References
-
- Agrawal M, Emanuel EJ (2003) Ethics of phase 1 oncology studies: reexamining the arguments and data. JAMA 290(8): 1075–1082 - PubMed
-
- Arkenau HT, Barriuso J, Olmos D, Ang JE, de Bono J, Judson I, Kaye S (2009) Prospective validation of a prognostic score to improve patient selection for oncology Phase I trials. J Clin Oncol 27 (in press) - PubMed
-
- Banerji U, Bono J, Judson I, Kaye S, Workman P (2008) Biomarkers in early clinical trials: the committed and the skeptics. Clin Cancer Res 14(8): 2512; author reply 2513–2514 - PubMed
-
- Booth CM, Calvert AH, Giaccone G, Lobbezoo MW, Seymour LK, Eisenhauer EA (2008) Endpoints and other considerations in phase I studies of targeted anticancer therapy: recommendations from the task force on Methodology for the Development of Innovative Cancer Therapies (MDICT). Eur J Cancer 44(1): 19–24 - PubMed
-
- Bubley GJ, Carducci M, Dahut W, Dawson N, Daliani D, Eisenberger M, Figg WD, Freidlin B, Halabi S, Hudes G, Hussain M, Kaplan R, Myers C, Oh W, Petrylak DP, Reed E, Roth B, Sartor O, Scher H, Simons J, Sinibaldi V, Small EJ, Smith MR, Trump DL, Wilding G (1999) Eligibility and response guidelines for phase II clinical trials in androgen-independent prostate cancer: recommendations from the Prostate-Specific Antigen Working Group. J Clin Oncol 17(11): 3461–3467 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
