

International consensus for neuroblastoma molecular diagnostics: report from the International Neuroblastoma Risk Group (INRG) Biology Committee
- PMID: 19401703
- PMCID: PMC2694415
- DOI: 10.1038/sj.bjc.6605014
International consensus for neuroblastoma molecular diagnostics: report from the International Neuroblastoma Risk Group (INRG) Biology Committee
Abstract
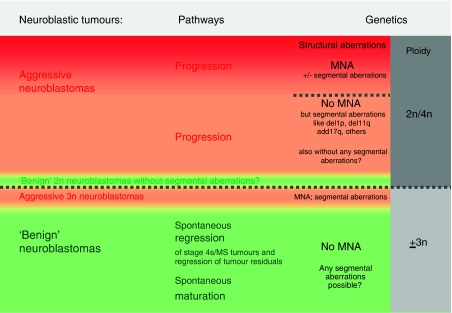
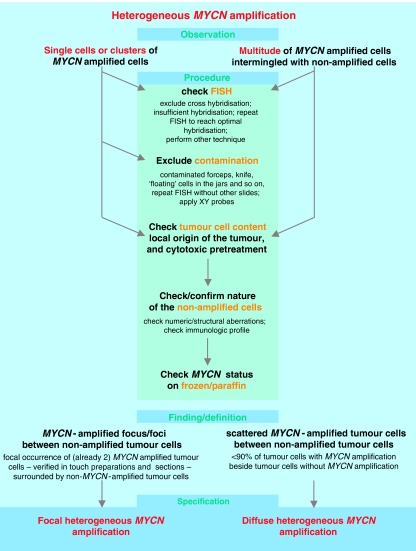
Neuroblastoma serves as a paradigm for utilising tumour genomic data for determining patient prognosis and treatment allocation. However, before the establishment of the International Neuroblastoma Risk Group (INRG) Task Force in 2004, international consensus on markers, methodology, and data interpretation did not exist, compromising the reliability of decisive genetic markers and inhibiting translational research efforts. The objectives of the INRG Biology Committee were to identify highly prognostic genetic aberrations to be included in the new INRG risk classification schema and to develop precise definitions, decisive biomarkers, and technique standardisation. The review of the INRG database (n=8800 patients) by the INRG Task Force finally enabled the identification of the most significant neuroblastoma biomarkers. In addition, the Biology Committee compared the standard operating procedures of different cooperative groups to arrive at international consensus for methodology, nomenclature, and future directions. Consensus was reached to include MYCN status, 11q23 allelic status, and ploidy in the INRG classification system on the basis of an evidence-based review of the INRG database. Standardised operating procedures for analysing these genetic factors were adopted, and criteria for proper nomenclature were developed. Neuroblastoma treatment planning is highly dependant on tumour cell genomic features, and it is likely that a comprehensive panel of DNA-based biomarkers will be used in future risk assignment algorithms applying genome-wide techniques. Consensus on methodology and interpretation is essential for uniform INRG classification and will greatly facilitate international and cooperative clinical and translational research studies.
Figures

References
-
- Ambros IM, Benard J, Boavida M, Bown N, Caron H, Combaret V, Couturier J, Darnfors C, Delattre O, Freeman-Edward J, Gambini C, Gross N, Hattinger CM, Luegmayr A, Lunec J, Martinsson T, Mazzocco K, Navarro S, Noguera R, O’Neill S, Potschger U, Rumpler S, Speleman F, Tonini GP, Valent A, Van Roy N, Amann G, De Bernardi B, Kogner P, Ladenstein R, Michon J, Pearson AD, Ambros PF (2003) Quality assessment of genetic markers used for therapy stratification. J Clin Oncol 21: 2077–2084 - PubMed
-
- Ambros IM, Zellner A, Roald B, Amann G, Ladenstein R, Printz D, Gadner H, Ambros PF (1996) Role of ploidy, chromosome 1p, and Schwann cells in the maturation of neuroblastoma [see comments]. N Engl J Med 334: 1505–1511 - PubMed
-
- Ambros PF, Ambros IM (2001) Pathology and biology guidelines for resectable and unresectable neuroblastic tumors and bone marrow examination guidelines. Med Pediatr Oncol 37: 492–504 - PubMed
-
- Ambros PF, Ambros IM, Strehl S, Bauer S, Luegmayr A, Kovar H, Ladenstein R, Fink FM, Horcher E, Printz G, Mutz I, Schilling F, Urban C, Gadner H (1995) Regression and progression in neuroblastoma. Does genetics predict tumour behaviour? Eur J Cancer 31A: 510–515 - PubMed
-
- Ambros PF, Mehes G, Hattinger C, Ambros IM, Luegmayr A, Ladenstein R, Gadner H (2001) Unequivocal identification of disseminated tumor cells in the bone marrow by combining immunological and genetic approaches—functional and prognostic information. Leukemia 15: 275–277 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
