

A single-dose combination therapy that both prevents and treats anthrax infection
- PMID: 19402202
- PMCID: PMC6335648
- DOI: 10.1016/j.vaccine.2009.01.094
A single-dose combination therapy that both prevents and treats anthrax infection
Abstract
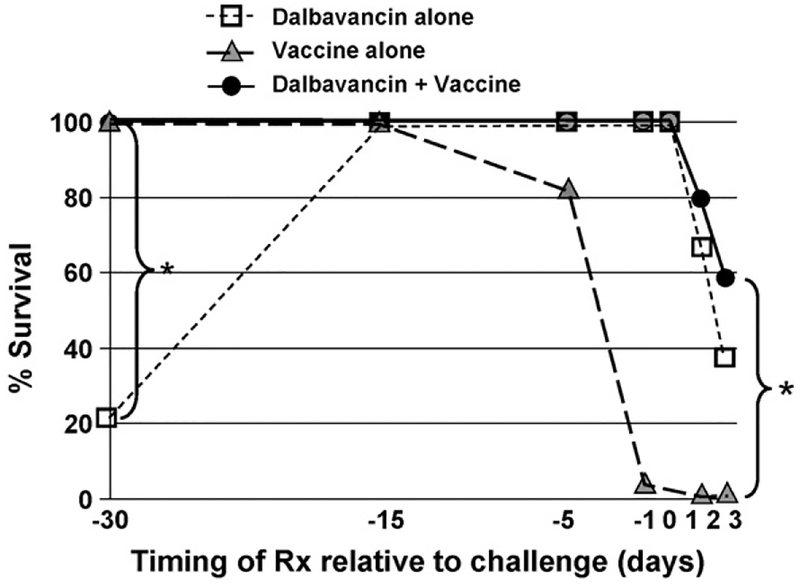
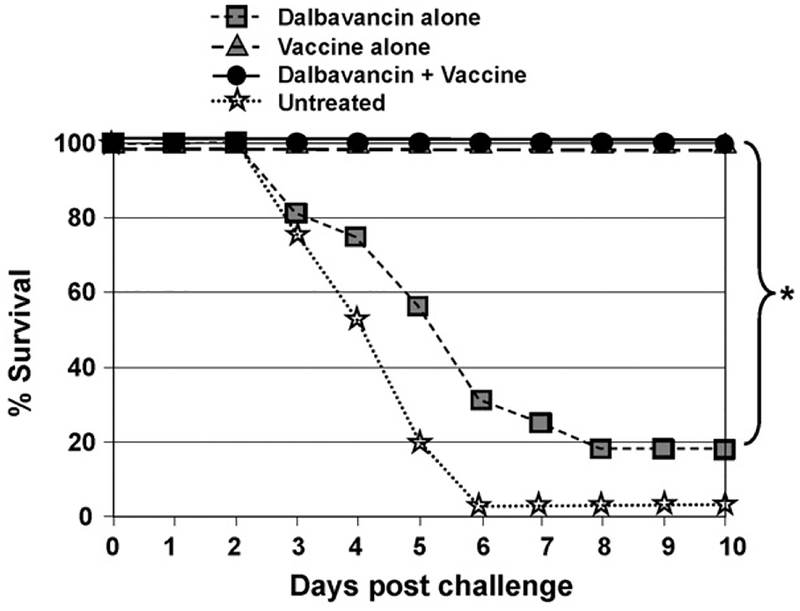
Exposure to anthrax leaves susceptible hosts at prolonged risk of infection since spores can persist in vivo for months before germinating to cause life-threatening disease. Anthrax vaccine adsorbed (AVA, the licensed US vaccine) induces immunity too slowly to protect susceptible individuals post-exposure. Antibiotics prevent the proliferation of vegetative bacilli but do not block latent spores from germinating. Thus, anthrax-exposed individuals must remain on antibiotic therapy for months to eliminate the threat posed by delayed spore germination. Unfortunately, long-term antibiotic treatment is poorly tolerated and frequently discontinued. This work explores whether administering a single dose of a long-acting antibiotic (Dalbavancin) combined with a rapidly immunogenic vaccine/adjuvant combination can provide seamless protection from anthrax with minimal patient compliance. Results show that significant protection is achieved by delivering a single dose of this therapeutic combination any time before through 3 days after anthrax exposure.
Figures
References
-
- Hanna P Anthrax pathogenesis and host response. Curr Top Microbiol Immunol 1998;225:13–35. - PubMed
-
- Lane HC, Montagne JL, Fauci AS. Bioterrorism: a clear and present danger. Nat Med 2001;7(December (12)):1271–3. - PubMed
-
- Ross JM. The pathogenesis of anthrax following the administration of spores by the respiratory route. J Pathol Bacteriol 1957;73:485–94.
-
- Glassman HN. Industrial inhalation anthrax: discussion. Bateriol Rev 1966;30:657–9. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
