

The influence of clinical information in the histopathologic diagnosis of melanocytic skin neoplasms
- PMID: 19404399
- PMCID: PMC2671836
- DOI: 10.1371/journal.pone.0005375
The influence of clinical information in the histopathologic diagnosis of melanocytic skin neoplasms
Erratum in
- PLoS One. 2009;4(6). doi: 10.1371/annotation/512cb17b-934c-4a06-9dbb-114d43052a2b doi: 10.1371/annotation/512cb17b-934c-4a06-9dbb-114d43052a2b
Abstract
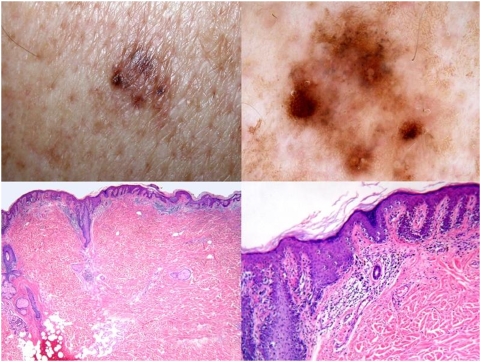
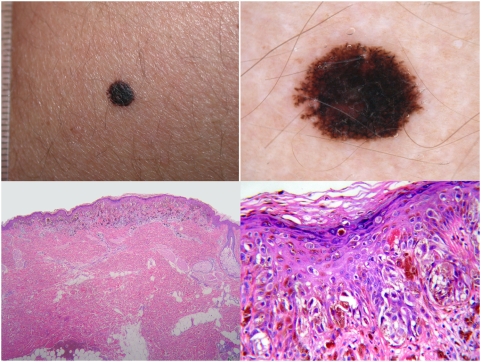
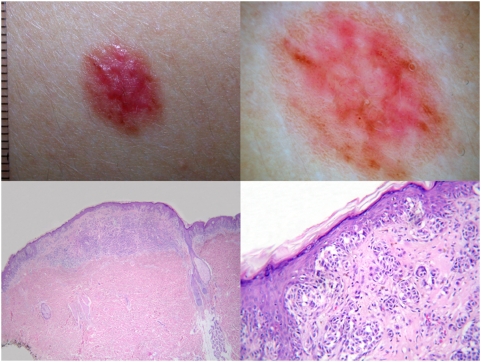
Background: We tested the relevance of clinical information in the histopathologic evaluation of melanocytic skin neoplasm (MSN).
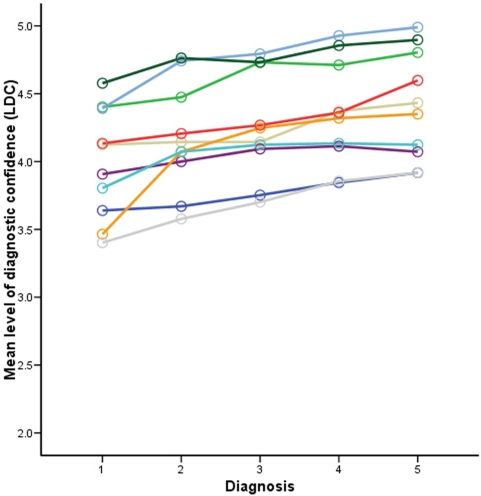
Methods: Histopathologic specimens from 99 clinically atypical MSN were circulated among ten histopathologists; each case had clinical information available in a database with a five-step procedure (no information; age/sex/location; clinical diagnosis; clinical image; dermoscopic image); each step had a histopathologic diagnosis (D1 through D5); each diagnostic step had a level of diagnostic confidence (LDC) ranging from 1 (no diagnostic certainty) to 5 (absolute diagnostic certainty). The comparison of the LDC was employed with an analysis of variance (ANOVA) for repeated measures.
Findings: In D1 (no information), 36/99 cases (36.3%) had unanimous diagnosis; in D5 (full information available), 51/99 cases (51.5%) had unanimous diagnosis (p for difference between proportions <0.001). The observer agreement expressed as kappa increased significantly from D1 to D5. The mean LDC linearly increased for each observer from D1 through D5 (p for linear trend <0.001). On average, each histopathologist changed his initial diagnosis in 7 cases (range: 2-23). Most diagnostic changes were in D2 (age/sex/location).
Interpretation: The histopathologic criteria for the diagnosis of MSN can work as such, but the final histopathologic diagnosis is a clinically-aided interpretation. Clinical data sometimes reverse the initial histopathologic evaluation.
Conflict of interest statement
Figures
References
-
- Ferrara G, Argenziano G, Soyer HP, Corona R, Sera F, et al. Dermoscopic and histopathologic diagnosis of equivocal melanocytic skin lesions. An interdisciplinary study on 107 cases. Cancer. 2002;95:1094–1100. - PubMed
-
- Corona R, Mele A, Amini M, De Rosa G, Coppola G, et al. Interobserver variability on the histopathologic diagnosis of cutaneous melanoma and other pigmented skin lesions. J Clin Oncol. 1996;14:1218–1223. - PubMed
-
- Farmer ER, Gonin R, Hanna MP. Discordance in the histopathologic diagnosis of melanoma and melanocytic nevi between expert pathologists. Hum Pathol. 1996;27:528–531. - PubMed
-
- Cerroni L, Kerl H. Tutorial on melanocytic lesions. Am J Dermatopathol. 2001;23:237–241. - PubMed
-
- Lowes MA, Norris D, Whitfeld M. Benign melanocytic proliferative nodule within a congenital naevus. Australas J Dermatol. 2000;41:109–111. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
