

Obstructive sleep apnea, immuno-inflammation, and atherosclerosis
- PMID: 19404644
- PMCID: PMC3937574
- DOI: 10.1007/s00281-009-0148-5
Obstructive sleep apnea, immuno-inflammation, and atherosclerosis
Abstract
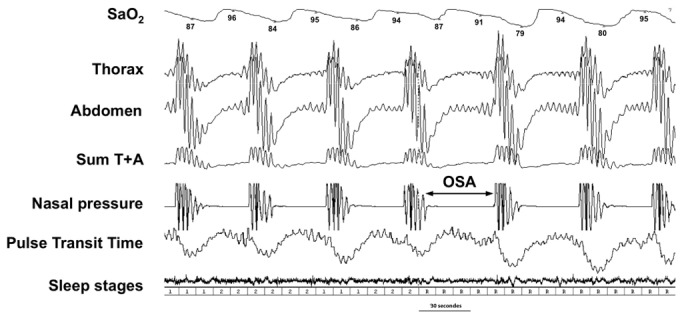
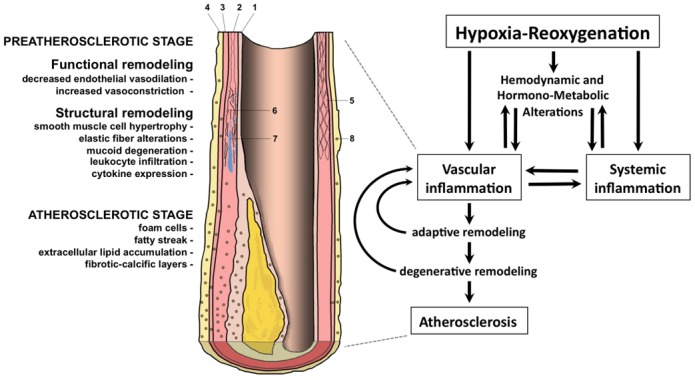
Obstructive sleep apnea (OSA) is a highly prevalent sleep disorder leading to cardiovascular and metabolic complications. OSA is also a multicomponent disorder, with intermittent hypoxia (IH) as the main trigger for the associated cardiovascular and metabolic alterations. Indeed, recurrent pharyngeal collapses during sleep lead to repetitive sequences of hypoxia-reoxygenation. This IH induces several consequences such as hemodynamic, hormonometabolic, oxidative, and immuno-inflammatory alterations that may interact and aggravate each other, resulting in artery changes, from adaptive to degenerative atherosclerotic remodeling. Atherosclerosis has been found in OSA patients free of other cardiovascular risk factors and is related to the severity of nocturnal hypoxia. Early stages of artery alteration, including functional and structural changes, have been evidenced in both OSA patients and rodents experimentally exposed to IH. Impaired vasoreactivity with endothelial dysfunction and/or increased vasoconstrictive responses due to sympathetic, endothelin, and renin-angiotensin systems have been reported and also contribute to vascular remodeling and inflammation. Oxidative stress, inflammation, and vascular remodeling can be directly triggered by IH, further aggravated by the OSA-associated hormonometabolic alterations, such as insulin resistance, dyslipidemia, and adipokine imbalance. As shown in OSA patients and in the animal model, genetic susceptibility, comorbidities (obesity), and life habits (high fat diet) may aggravate atherosclerosis development or progression. The intimate molecular mechanisms are still largely unknown, and their understanding may contribute to delineate new targets for prevention strategies and/or development of new treatment of OSA-related atherosclerosis, especially in patients at risk for cardiovascular disease.
Figures
References
-
- Malhotra A, White DP. Obstructive sleep apnoea. Lancet. 2002;360(9328):237–45. - PubMed
-
- Somers VK, et al. Sleep apnea and cardiovascular disease: an American Heart Association/american College Of Cardiology Foundation Scientific Statement from the American Heart Association Council for High Blood Pressure Research Professional Education Committee, Council on Clinical Cardiology, Stroke Council, and Council On Cardiovascular Nursing. In collaboration with the National Heart, Lung, and Blood Institute National Center on Sleep Disorders Research (National Institutes of Health) Circulation. 2008;118(10):1080–111. - PubMed
-
- Mayer P, et al. Relationship between body mass index, age and upper airway measurements in snorers and sleep apnoea patients. Eur Respir J. 1996;9(9):1801–9. - PubMed
-
- White DP. Pathogenesis of obstructive and central sleep apnea. Am J Respir Crit Care Med. 2005;172(11):1363–70. - PubMed
-
- Horner RL. Contributions of passive mechanical loads and active neuromuscular compensation to upper airway collapsibility during sleep. J Appl Physiol. 2007;102(2):510–2. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
