

Comparison of single-level L4-L5 versus L5-S1 lumbar disc replacement: results and prognostic factors
- PMID: 19404688
- PMCID: PMC2899612
- DOI: 10.1007/s00586-009-0992-y
Comparison of single-level L4-L5 versus L5-S1 lumbar disc replacement: results and prognostic factors
Abstract
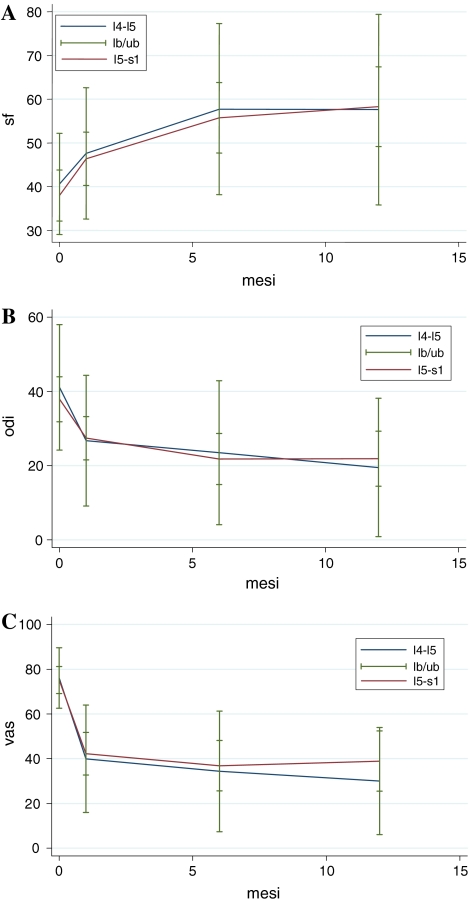
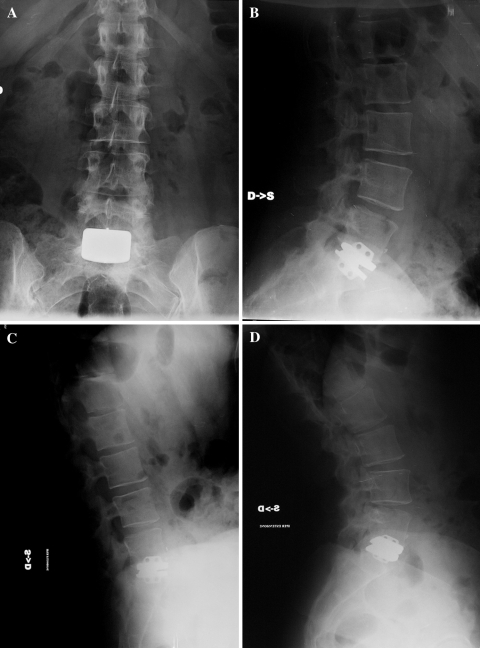
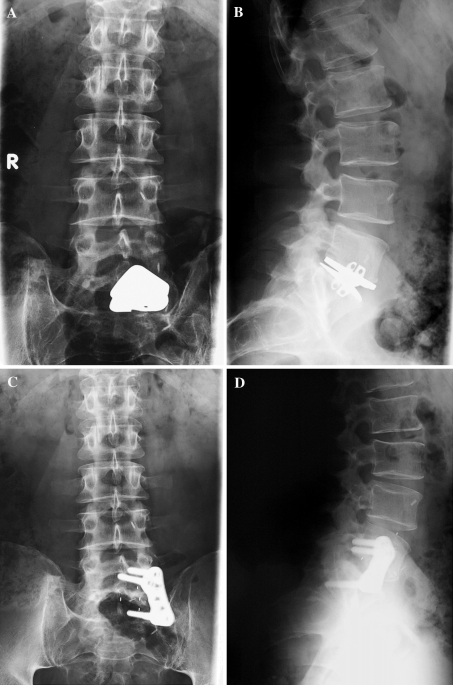
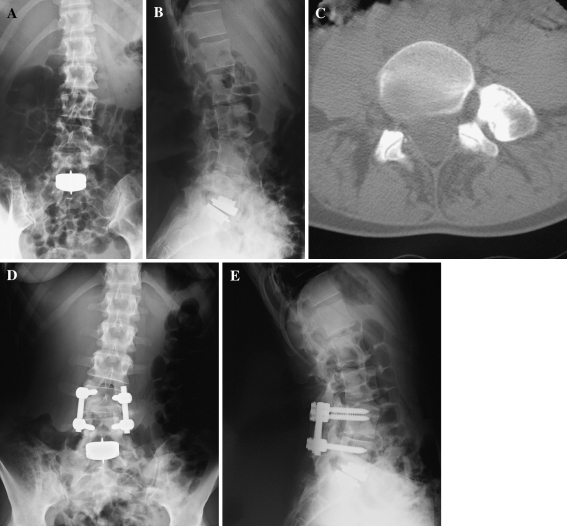
The aim of our prospective non-randomized clinical study was to analyze operative data, short-term results, safety, efficacy, complications, and prognostic factors for single-level total lumbar disc replacement (TLDR), and to compare results between different levels (L4-L5 vs. L5-S1). Thirty-six patients with single-level L4-L5 or L5-S1 TLDR, with 1-year minimum follow-up (FU), had complete clinical [SF36, visual analog scale (VAS), Oswestry Disability Index (ODI)] and radiological data, and were included in our study. Mean FU was 38.67 +/- 17.34 months. Replaced level was L4-L5 in 12 (33.3%) cases, and L5-S1 in 24 cases (66.7%). Mean age at diagnosis was 41.17 +/- 7.14 years. 24 (66.7%) were females and 12 (33.3%) were males. Statistical analyses were assessed using t tests or Mann-Whitney test for continuous variables and Chi-square test or Fisher's exact test analyses for categorical variables. Univariate linear regression and binary logistic regression analyses were utilized to evaluate the relationship between surgical outcomes and covariates (gender, age, etiology, treated level, pre-operative SF36, ODI, and VAS). Mean operative time was 147.03 +/- 30.03 min. Mean hospital stay was 9.69 +/- 5.39 days, and mean return to ambulation was 4.31 +/- 1.17 days. At 1-year FU, patients revealed a statistical significant improvement in VAS pain (P = 0.000), ODI lumbar function (P = 0.000), and SF36 general health status (P = 0.000). Single-level TLDR is a good alternative to fusion for chronic discogenic low back pain refractory to conservative measures. Our study confirmed satisfactory clinical results for monosegmental L4-L5 and L5-S1 disc prosthesis, with no difference between the two different levels for SF36 (P = 0.217), ODI (P = 0.527), and VAS (P = 0.269). However, replacement of the L4-L5 disc is affected by an increased risk of complication (P = 0.000). There were no prognostic factors for intraoperative blood loss or return to ambulation. Age (P = 0.034) was the only prognostic factor for operative time. Hospital stay was affected by level (P = 0.036) and pre-op VAS (P = 0.006), while complications were affected by the level (P = 0.000) and pre-op ODI (P = 0.049). Complete pre-operative assessment (in particular VAS and ODI questionnaires) is important because more debilitating patients will have more hospital stay and higher complications or complaints. Patients had to be informed that complications, possibly severe, are particularly frequent (80.6%).
Figures

Similar articles
-
A short report comparing outcomes between L4/L5 and L5/S1 single-level discectomy surgery.J Spinal Disord Tech. 2010 Feb;23(1):40-2. doi: 10.1097/BSD.0b013e3181b38537. J Spinal Disord Tech. 2010. PMID: 20134287
-
Hybrid construct for two levels disc disease in lumbar spine.Eur Spine J. 2010 Feb;19(2):290-6. doi: 10.1007/s00586-009-1182-7. Epub 2009 Nov 4. Eur Spine J. 2010. PMID: 19888610 Free PMC article.
-
Anterior Lumbar Interbody Fusion for Degenerative Discogenic Low Back Pain: Evaluation of L4-S1 Fusion.Medicine (Baltimore). 2015 Oct;94(43):e1851. doi: 10.1097/MD.0000000000001851. Medicine (Baltimore). 2015. PMID: 26512594 Free PMC article.
-
Comparison of Full Endoscopic Lumbar Diskectomy Using the Transforaminal Approach versus Interlaminar Approach for L5-S1 Lumbar Disk Herniation Treatment: A Meta-Analysis.J Neurol Surg A Cent Eur Neurosurg. 2024 Sep;85(5):501-512. doi: 10.1055/a-2053-8365. Epub 2023 Mar 14. J Neurol Surg A Cent Eur Neurosurg. 2024. PMID: 36918155
-
Spontaneous regression of a large sequestered lumbar disc herniation: a case report and literature review.J Int Med Res. 2021 Nov;49(11):3000605211058987. doi: 10.1177/03000605211058987. J Int Med Res. 2021. PMID: 34812080 Free PMC article. Review.
Cited by
-
In silico evaluation of a new composite disc substitute with a L3-L5 lumbar spine finite element model.Eur Spine J. 2012 Jun;21 Suppl 5(Suppl 5):S675-87. doi: 10.1007/s00586-011-1716-7. Epub 2011 Mar 5. Eur Spine J. 2012. PMID: 21380572 Free PMC article.
-
We Need to Talk about Lumbar Total Disc Replacement.Int J Spine Surg. 2018 Aug 3;12(2):201-240. doi: 10.14444/5029. eCollection 2018 Apr. Int J Spine Surg. 2018. PMID: 30276080 Free PMC article.
-
Radiographic Analysis of the Lumbosacral Juncture: Is There a Critical Sacral Angle for Total Disc Replacement?Asian Spine J. 2017 Apr;11(2):249-255. doi: 10.4184/asj.2017.11.2.249. Epub 2017 Apr 12. Asian Spine J. 2017. PMID: 28443169 Free PMC article.
-
ISASS Policy Statement - Lumbar Artificial Disc.Int J Spine Surg. 2015 Mar 12;9:7. doi: 10.14444/2007. eCollection 2015. Int J Spine Surg. 2015. PMID: 25785243 Free PMC article.
-
Sagittal plane rotation center of lower lumbar spine during a dynamic weight-lifting activity.J Biomech. 2016 Feb 8;49(3):371-5. doi: 10.1016/j.jbiomech.2015.12.029. Epub 2015 Dec 29. J Biomech. 2016. PMID: 26805460 Free PMC article.
References
-
- Bertagnoli R, Marnay T, Mayer HM, editors. Total disc replacement. Tuttlingen: Spine Solutions GmbH; 2003.
-
- Bertagnoli R, Yue JJ, Shah RV, Nanieva R, Pfeiffer F, Fenk-Mayer A, Kershaw T, Husted DS. The treatment of disabling single-level lumbar discogenic low back pain with total disc arthroplasty utilizing the Prodisc prosthesis: a prospective study with 2-year minimum follow-up. Spine. 2005;30:2230–2236. doi: 10.1097/01.brs.0000182217.87660.40. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
