

Reduced hospital stay, morphine consumption, and pain intensity with local infiltration analgesia after unicompartmental knee arthroplasty
- PMID: 19404806
- PMCID: PMC2823175
- DOI: 10.3109/17453670902930008
Reduced hospital stay, morphine consumption, and pain intensity with local infiltration analgesia after unicompartmental knee arthroplasty
Abstract
Background and purpose: The degree of postoperative pain is usually moderate to severe following knee arthroplasty. We investigated the efficacy of local administration of analgesics into the operating area, both intraoperatively and postoperatively.
Methods: 40 patients undergoing unicompartmental knee arthroplasty (UKA) were randomized into 2 groups in a double-blind study (ClinicalTrials.gov identifier: NCT00653926). In group A (active), 200 mg ropivacaine, 30 mg ketorolac, and 0.5 mg epinephrine (total volume 106 mL) were infiltrated intraoperatively into the soft tissue, while in group P (placebo), no injections were given. 21 hours postoperatively, 150 mg ropivacain, 30 mg ketorolac, and 0.1 mg epinephrine were injected intraarticularly via a catheter in group A, whereas patients in group P were injected with the same volume of saline (22 mL).
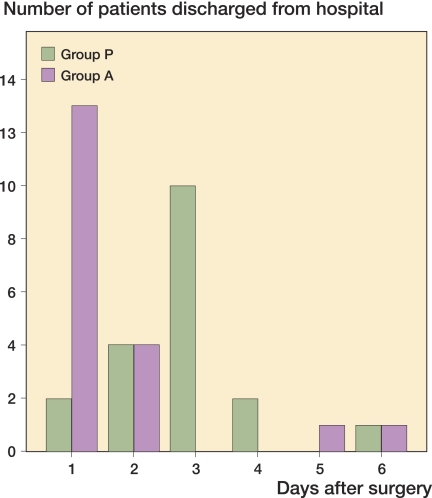
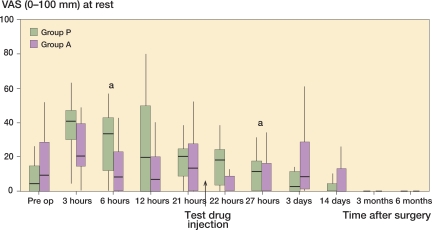
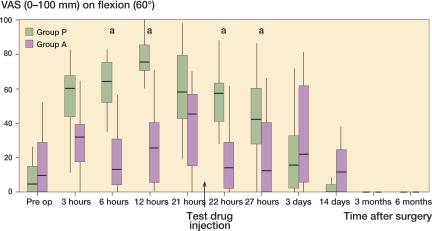
Results: Median hospital stay was shorter in group A than in group P: 1 (1-6) days as opposed to 3 (1-6) days (p < 0.001). Postoperative pain in group A was statistically significantly lower at rest after 6 h and 27 h and on movement after 6, 12, 22, and 27 h. Morphine consumption was statistically significantly lower in group A for the first 48 h, resulting in a lower frequency of nausea, pruritus, and sedation. Postoperatively, there were improved functional scores (Oxford knee score and EQ-5D) in both groups relative to the corresponding preoperative values.
Interpretation: Local injection of analgesics periarticularly at the end of the operation and intraarticularly at 21 h postoperatively provided excellent pain relief and earlier home discharge following UKA. There was a high degree of patient satisfaction in both groups after 6 months (Clinical Trials.gov: NCT 00653926).
Figures

References
-
- Axelsson K, Johanzon E, Essving P, Weckstrom J, Ekback G. Postoperative extradural analgesia with morphine and ropivacaine. A double–blind comparison between placebo and ropivacaine 10 mg/h or 16 mg/h. Acta Anaesthesiol Scand. 2005;49:1191–9. - PubMed
-
- Beard DJ, Murray DW, Rees JL, Price AJ, Dodd CA. Accelerated recovery for unicompartmental knee replacement––a feasibility study. Knee. 2002;9:221–4. - PubMed
-
- Berend KR, Lombardi AVJR. Liberal indications for minimally invasive oxford unicondylar arthroplasty provide rapid functional recovery and pain relief. Surg Technol Int. 2007;16:193–7. - PubMed
-
- Carlsson LV, Albrektsson BE, Regner LR. Minimally invasive surgery vs conventional exposure using the Miller–Galante unicompartmental knee arthroplasty: a randomized radiostereometric study. J Arthroplasty. 2006;21:151–6. - PubMed
-
- Fransen M, Edmonds J. Gait variables: appropriate objective outcome measures in rheumatoid arthritis. Rheumatology (Oxford) 1999;38:663–7. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical