

Lower thoracic spinal cord stimulation to restore cough in patients with spinal cord injury: results of a National Institutes of Health-sponsored clinical trial. Part I: methodology and effectiveness of expiratory muscle activation
- PMID: 19406289
- PMCID: PMC2813808
- DOI: 10.1016/j.apmr.2008.11.013
Lower thoracic spinal cord stimulation to restore cough in patients with spinal cord injury: results of a National Institutes of Health-sponsored clinical trial. Part I: methodology and effectiveness of expiratory muscle activation
Abstract
Objective: Evaluation of the capacity of lower thoracic spinal cord stimulation (SCS) to activate the expiratory muscles and generate large airway pressures and high peak airflows characteristic of cough, in subjects with tetraplegia.
Design: Clinical trial.
Setting: Inpatient hospital setting for electrode insertion; outpatient setting for measurement of respiratory pressures; home setting for application of SCS.
Participants: Subjects (N=9; 8 men, 1 woman) with cervical spinal cord injury and weak cough.
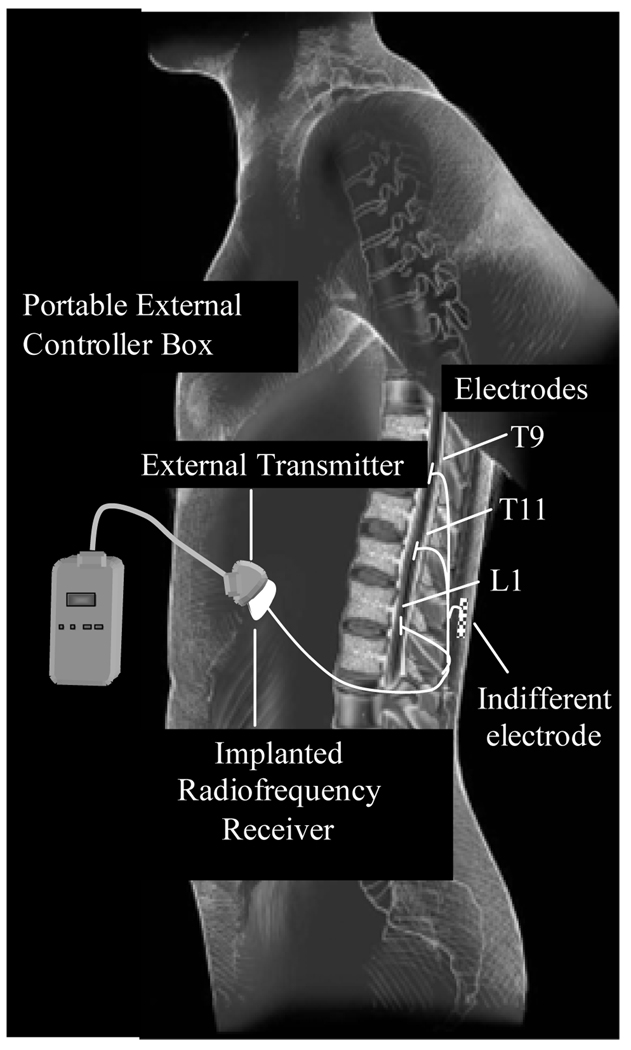
Interventions: A fully implantable electrical stimulation system was surgically placed in each subject. Partial hemilaminectomies were made to place single-disk electrodes in the epidural space at the T9, T11, and L1 spinal levels. A radiofrequency receiver was placed in a subcutaneous pocket over the anterior portion of the chest wall. Electrode wires were tunneled subcutaneously and connected to the receiver. Stimulation was applied by activating a small portable external stimulus controller box powered by a rechargeable battery to each electrode lead alone and in combination.
Main outcome measures: Peak airflow and airway pressure generation achieved with SCS.
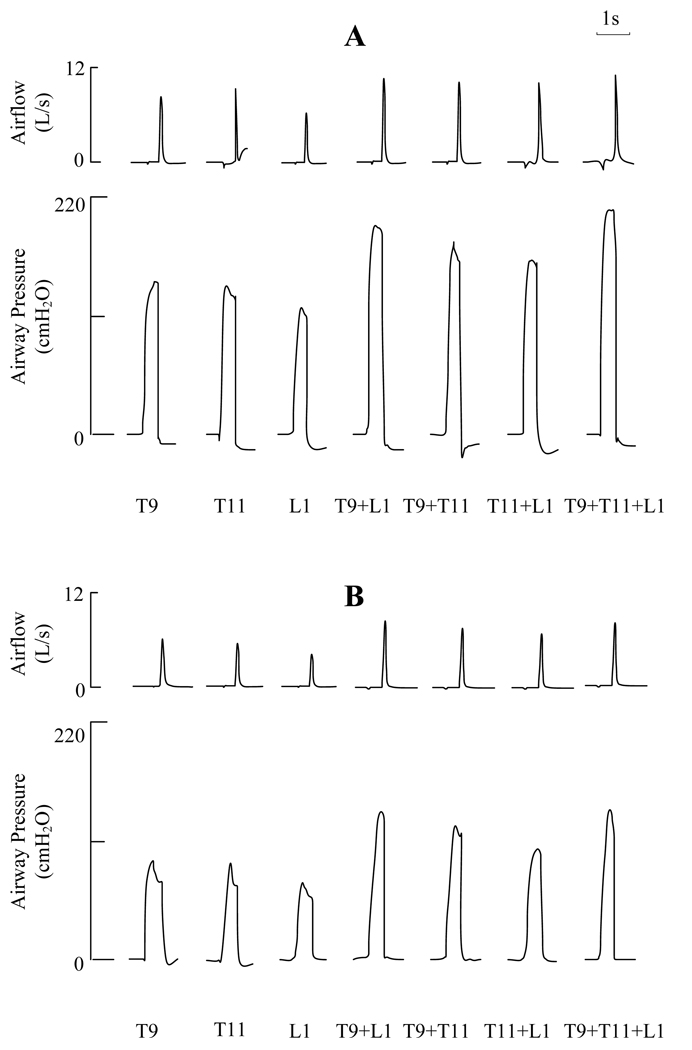
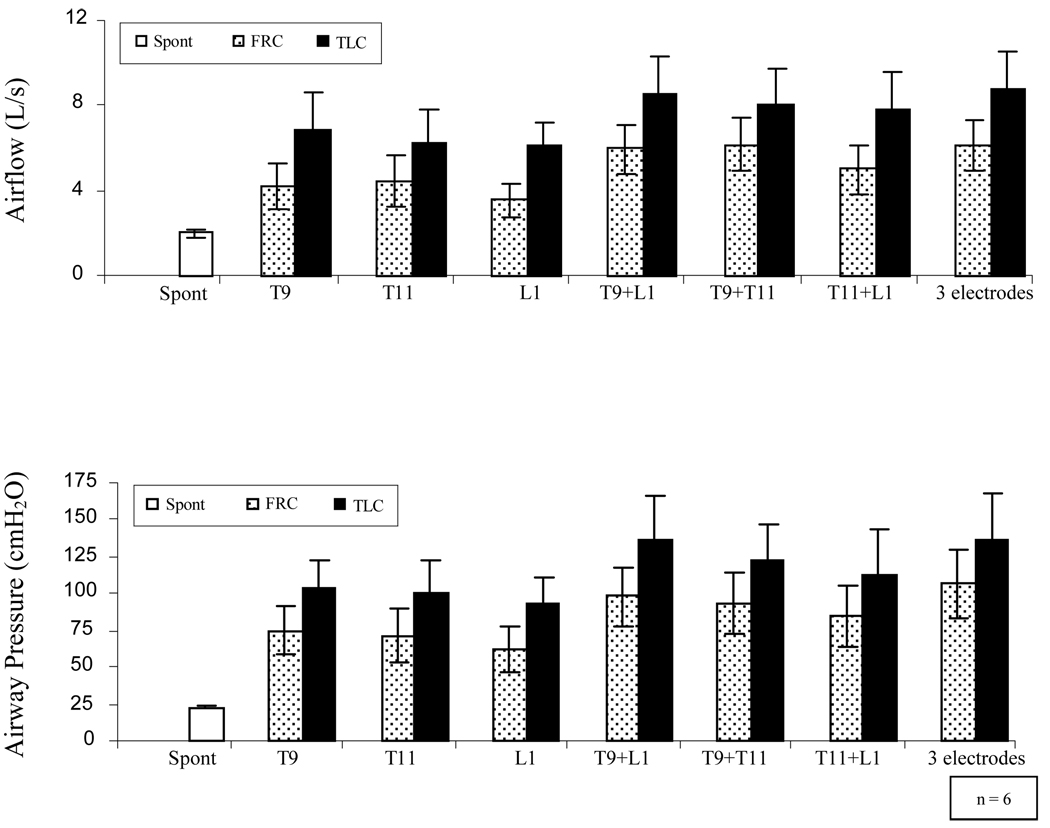
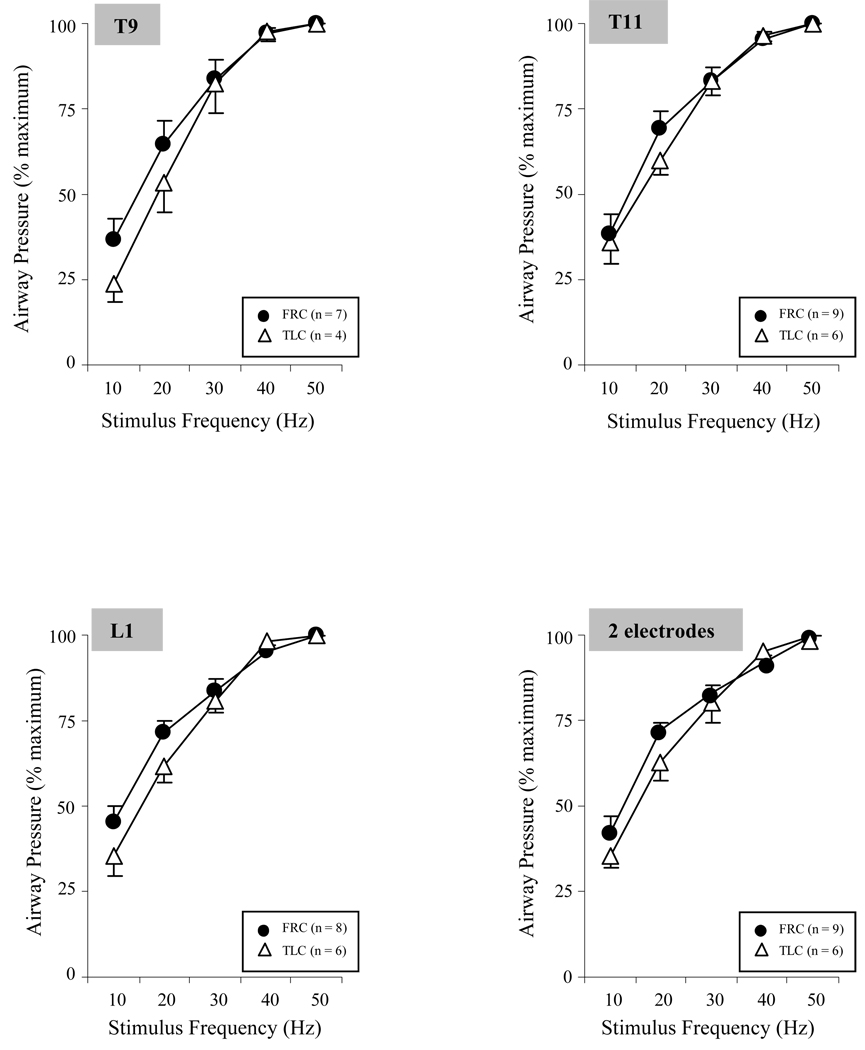
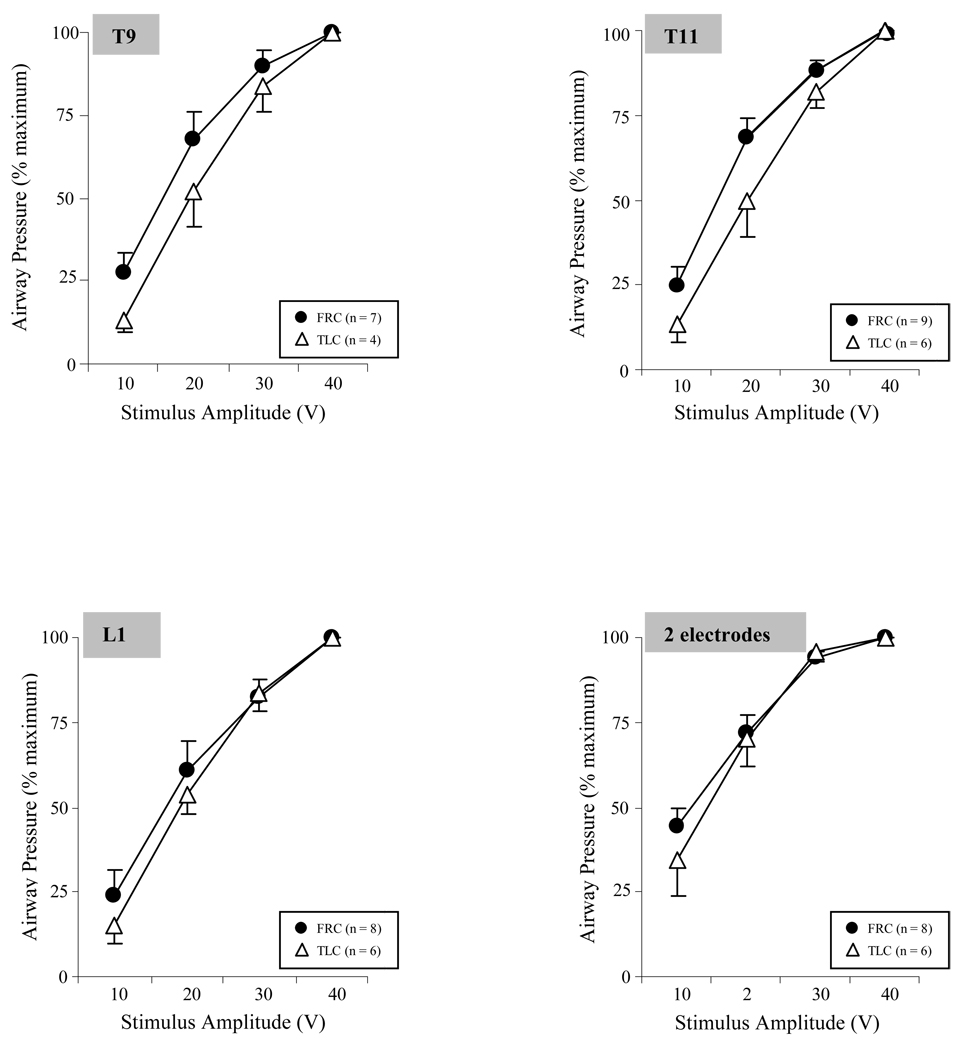
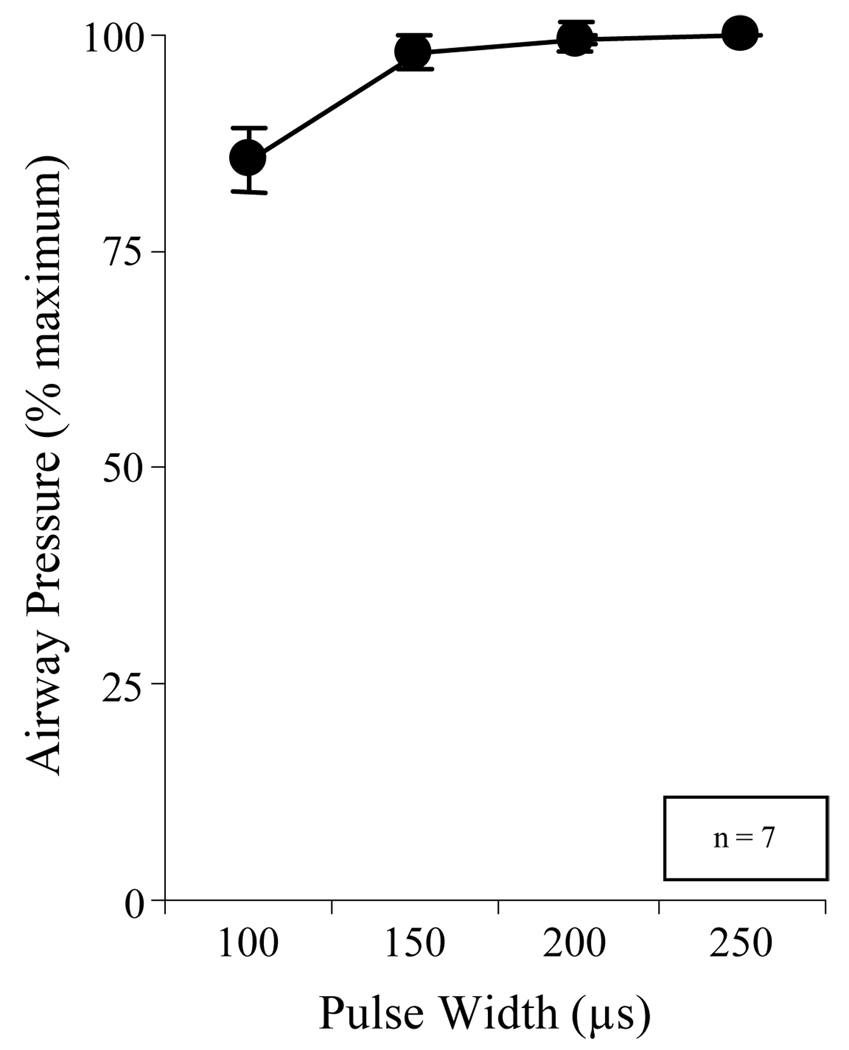
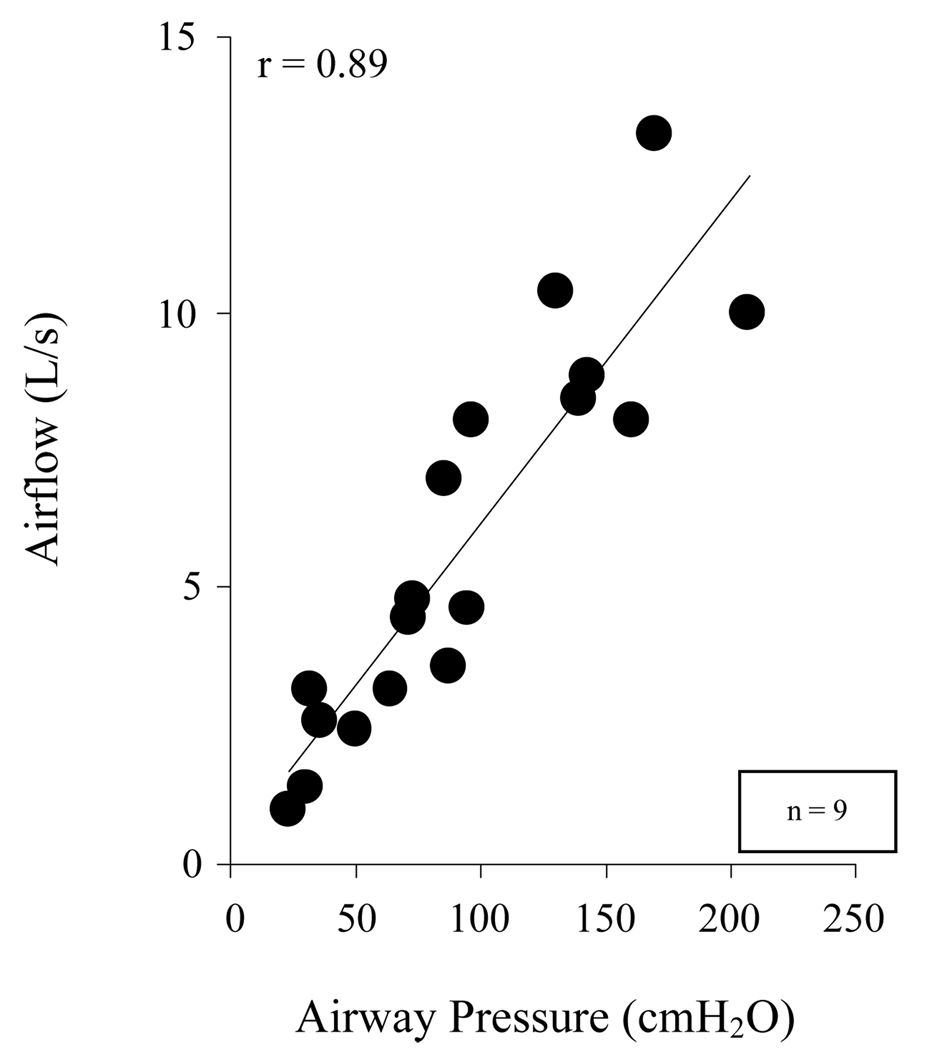
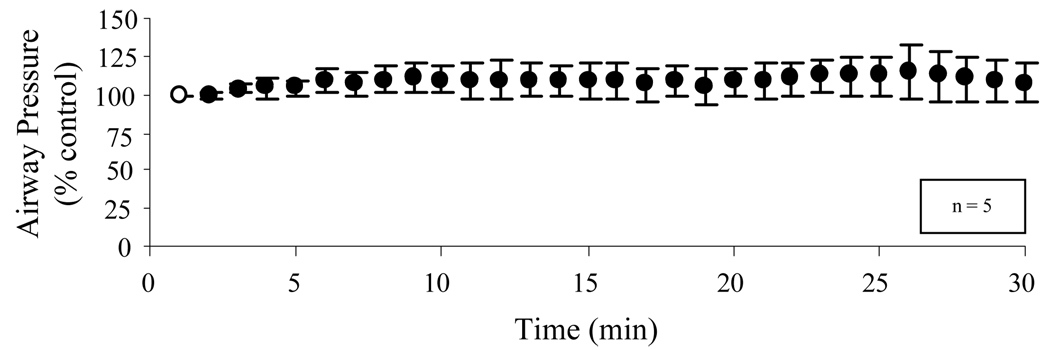
Results: Supramaximal SCS resulted in high peak airflow rates and large airway pressures during stimulation at each electrode lead. Maximum peak airflow rates and airway pressures were achieved with combined stimulation of any 2 leads. At total lung capacity, mean maximum peak airflow rates and airway pressure generation were 8.6+/-1.8 (mean +/- SE) L/s and 137+/-30 cmH2O (mean +/- SE), respectively.
Conclusions: Lower thoracic SCS results in near maximum activation of the expiratory muscles and the generation of high peak airflow rates and positive airway pressures in the range of those observed with maximum cough efforts in healthy persons.
Trial registration: ClinicalTrials.gov NCT00116337.
Figures
References
-
- DeTroyer A, Estenne M, Heilporn A. Mechanism of active expiration in tetraplegic subjects. N Engl J Med. 1986;314:740–744. - PubMed
-
- Estenne M, DeTroyer A. Cough in tetraplegic subjects: an active process. Ann Intern Med. 1990;112:22–28. - PubMed
-
- Kelly BJ, Luce JM. The diagnosis and management of neuromuscular diseases causing respiratory failure. Chest. 1991;99:1485–1494. - PubMed
-
- McMichan JC, Michel L, Westbrook PR. Pulmonary dysfunction following traumatic quadriplegia: recognition, prevention and treatment. JAMA. 1980;243:528–531. - PubMed
-
- Carter RE. Respiratory aspects of spinal cord injury management. Paraplegia. 1987;25:262–266. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
