

Clinical effectiveness of coronary stents in elderly persons: results from 262,700 Medicare patients in the American College of Cardiology-National Cardiovascular Data Registry
- PMID: 19406337
- PMCID: PMC2841783
- DOI: 10.1016/j.jacc.2009.03.005
Clinical effectiveness of coronary stents in elderly persons: results from 262,700 Medicare patients in the American College of Cardiology-National Cardiovascular Data Registry
Abstract
Objectives: The aim of this study was to compare outcomes in older individuals receiving drug-eluting stents (DES) and bare-metal stents (BMS).
Background: Comparative effectiveness of DES relative to BMS remains unclear.
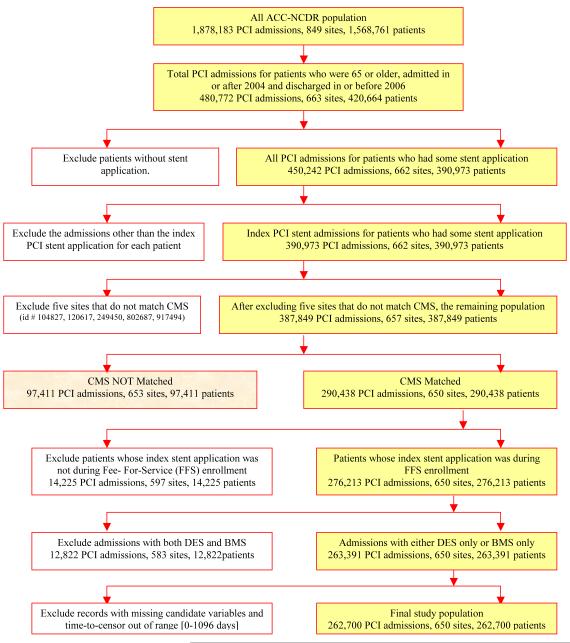
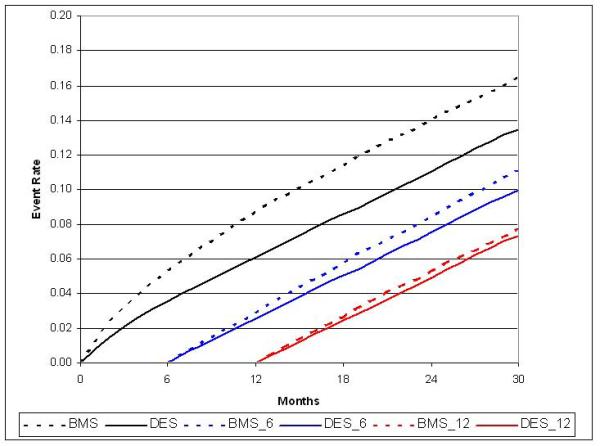
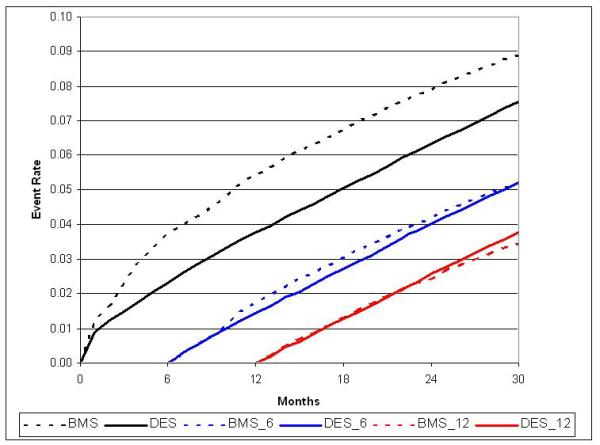
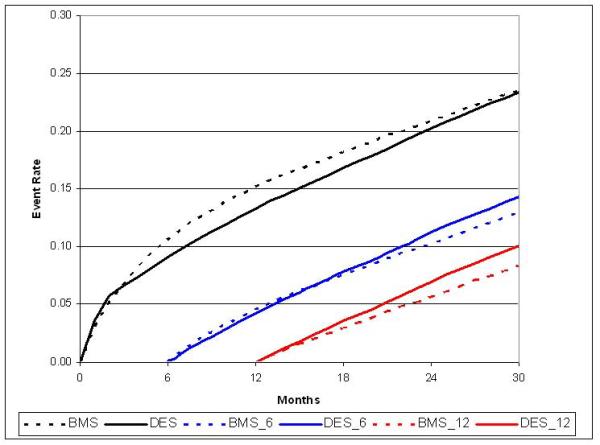
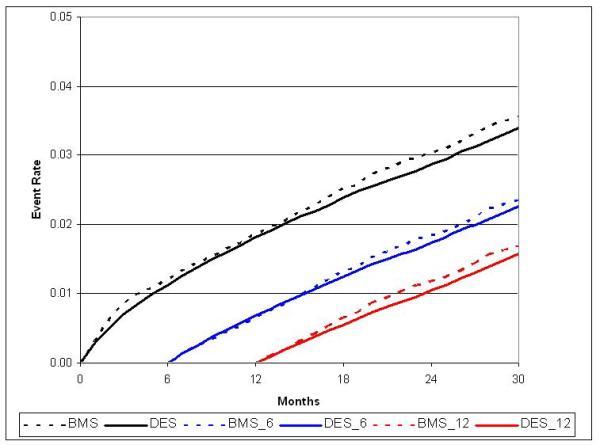
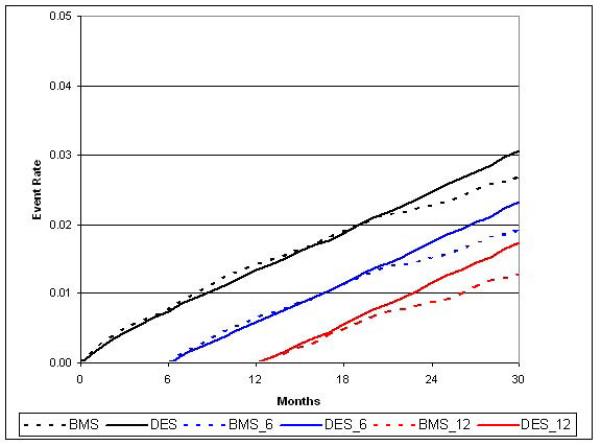
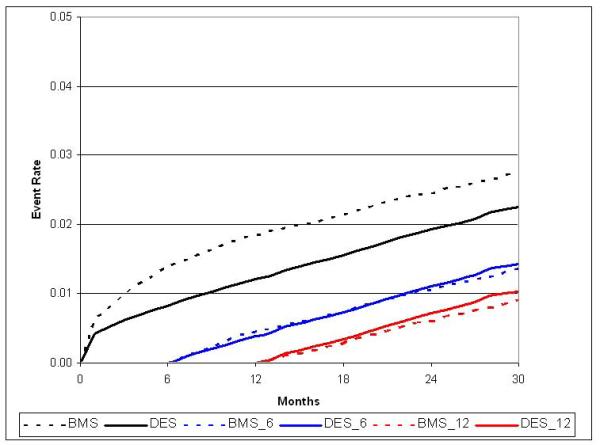
Methods: Outcomes were evaluated in 262,700 patients from 650 National Cardiovascular Data Registry sites during 2004 to 2006 with procedural registry data linked to Medicare claims for follow-up. Outcomes including death, myocardial infarction (MI), revascularization, major bleeding, stroke, death or MI, death or MI or revascularization, and death or MI or stroke were compared with estimated cumulative incidence rates with inverse probability weighted estimators and Cox proportional hazards ratios.
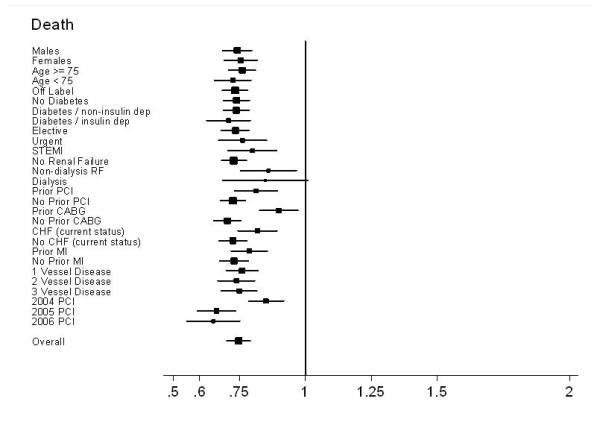
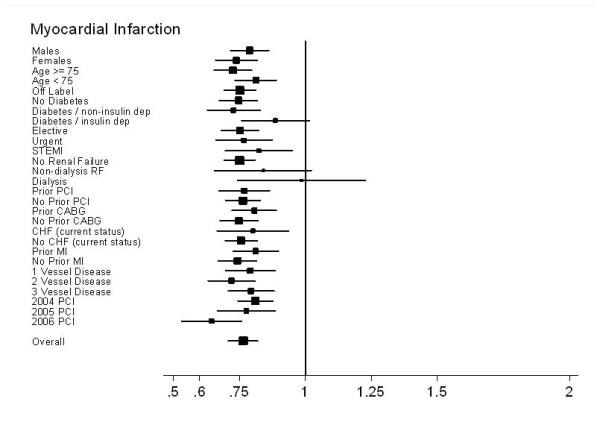
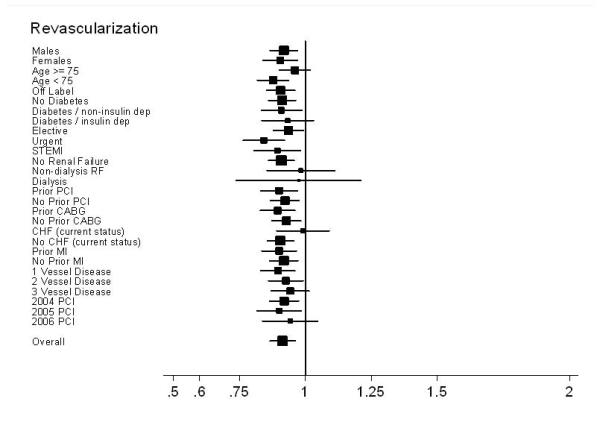
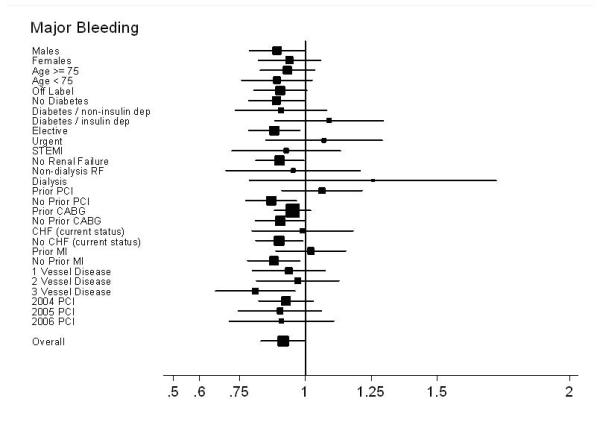
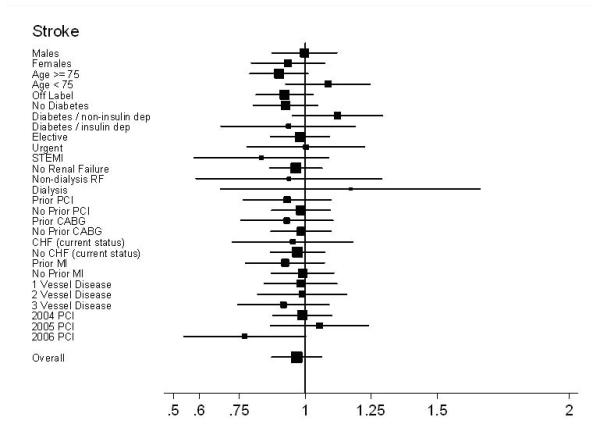
Results: The DES were implanted in 217,675 patients and BMS were implanted in 45,025. At 30 months, DES patients had lower unadjusted rates of death (12.9% vs. 17.9%), MI (7.3 of 100 patients vs. 10.0 of 100 patients), and revascularization (23.0 of 100 patients vs. 24.5 of 100 patients) with no difference in stroke or bleeding. After adjustment, DES patients had lower rates of death (13.5% vs. 16.5%, hazard ratio [HR]: 0.75, 95% confidence interval [CI]: 0.72 to 0.79, p < 0.001) and MI (7.5 of 100 patients vs. 8.9 of 100 patients, HR: 0.77, 95% CI: 0.72 to 0.81, p < 0.001), with minimal difference in revascularization (23.5 of 100 patients vs. 23.4 of 100 patients; HR: 0.91, 95% CI: 0.87 to 0.96), stroke (3.1 of 100 patients vs. 2.7 of 100 patients, HR: 0.97, 95% CI: 0.88 to 1.07), or bleeding (3.4 of 100 patients vs. 3.6 of 100 patients, HR: 0.91, 95% CI: 0.84 to 1.00). The DES survival benefit was observed in all subgroups analyzed and persisted throughout 30 months of follow-up.
Conclusions: In this largest ever real-world study, patients receiving DES had significantly better clinical outcomes than their BMS counterparts, without an associated increase in bleeding or stroke, throughout 30 months of follow-up and across all pre-specified subgroups.
Figures
References
-
- Stettler C, Wandel S, Allemann S, et al. Outcomes associated with drug-eluting and bare-metal stents: a collaborative network meta-analysis. The Lancet. 370:937–948. - PubMed
-
- Rao SV, Shaw RE, Brindis RG, et al. Patterns and outcomes of drug-eluting coronary stent use in clinical practice. American Heart Journal. 2006;152:321–326. - PubMed
-
- Virmani R, Guagliumi G, Farb A, et al. Localized Hypersensitivity and Late Coronary Thrombosis Secondary to a Sirolimus-Eluting Stent: Should We Be Cautious? Circulation. 2004;109:701–705. - PubMed
-
- McFadden EP, Stabile E, Regar E, et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. The Lancet. 364:1519–1521. - PubMed
-
- Camenzind E, Steg PG, Wijns W. A Cause for Concern. Circulation. 2007;115:1440–1455. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
