

Review
doi: 10.1177/0022034509333371.
Human papillomavirus and head and neck squamous cell carcinoma: recent evidence and clinical implications
Affiliations
- PMID: 19407148
- PMCID: PMC3317947
- DOI: 10.1177/0022034509333371
Item in Clipboard
Review
Human papillomavirus and head and neck squamous cell carcinoma: recent evidence and clinical implications
J Dent Res.
2009 Apr.
Abstract
Over the past 20 years, high-risk human papilloma-virus (HPV) infection has been established as a risk factor for developing head and neck squamous cell carcinoma, independent of tobacco and alcohol use. In particular, HPV is strongly associated with the development of oropharyngeal cancer and a small minority of oral cavity cancers. In this review, we summarize what is currently known about the biology of HPV, the mechanisms by which it effects malignant transformation, and the potential impact of HPV status on the clinical management of persons with head and neck cancer.
Figures

Oropharyngeal squamous cell carcinoma evaluated by routine hematoxylin and eosin staining (box 1), p16 immunostaining (box 2), and HPV-16 in situ hybridization (box 3). Tumor islands demonstrate characteristic basaloid appearance and lymphocytic infiltration.
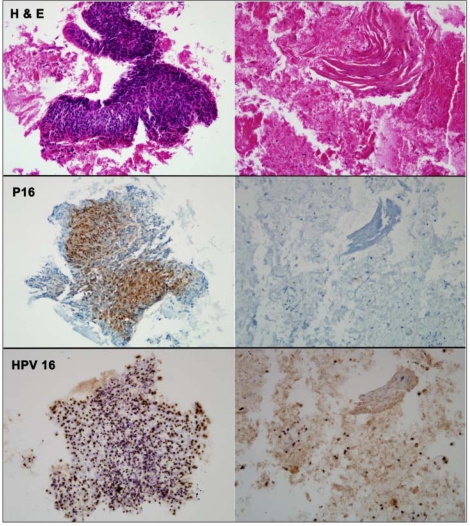
Fine-needle aspirate of a metastatic squamous cell carcinoma evaluated by routine hematoxylin and eosin staining (row 1), p16 immunostaining (row 2), and HPV in situ hybridization (row 3). A fragment of viable tumor (left column) is strongly p16-positive and HPV16-positive. In areas of cellular degeneration (right column), the tumor cells lose their p16 immunoreactivity, but retain their HPV16 hybridization signals. (Previously published in Begum et al., 2007. Used with permission.)
References
-
- Ahomadegbe JC, Barrois M, Fogel S, Le Bihan ML, Douc-Rasy S, Duvillard P, et al. (1995). High incidence of p53 alterations (mutation, deletion, overexpression) in head and neck primary tumors and metastases; absence of correlation with clinical outcome. Frequent protein overexpression in normal epithelium and in early non-invasive lesions. Oncogene 10:1217-1227 - PubMed
-
- Andrews E, Seaman WT, Webster-Cyriaque J. (2008). Oropharyngeal carcinoma in non-smokers and non-drinkers: a role for HPV. Oral Oncol (in press). - PubMed
-
- Begum S, Cao D, Gillison M, Zahurak M, Westra WH. (2005). Tissue distribution of human papillomavirus 16 DNA integration in patients with tonsillar carcinoma. Clin Cancer Res 11:5694-5699 - PubMed
-
- Begum S, Gillison ML, Nicol TL, Westra WH. (2007). Detection of human papillomavirus-16 in fine-needle aspirates to determine tumor origin in patients with metastatic squamous cell carcinoma of the head and neck. Clin Cancer Res 13:1186-1191 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
