

Exhaled air dispersion distances during noninvasive ventilation via different Respironics face masks
- PMID: 19411297
- PMCID: PMC7094372
- DOI: 10.1378/chest.09-0434
Exhaled air dispersion distances during noninvasive ventilation via different Respironics face masks
Abstract
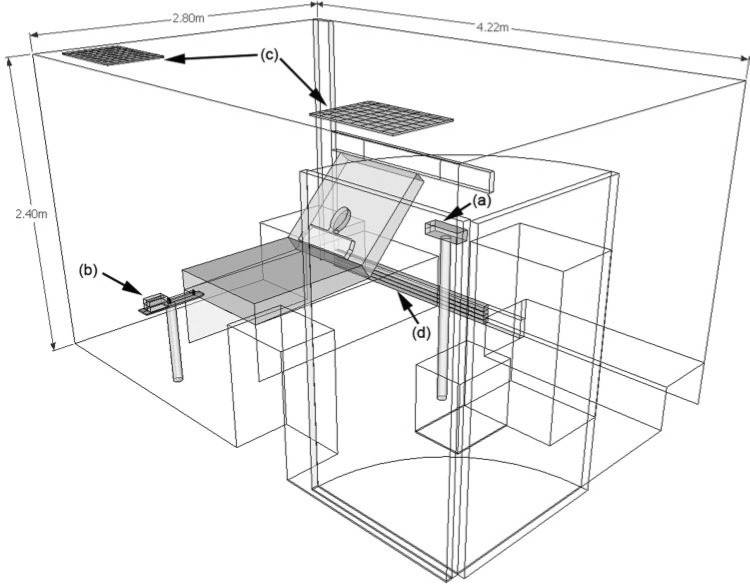
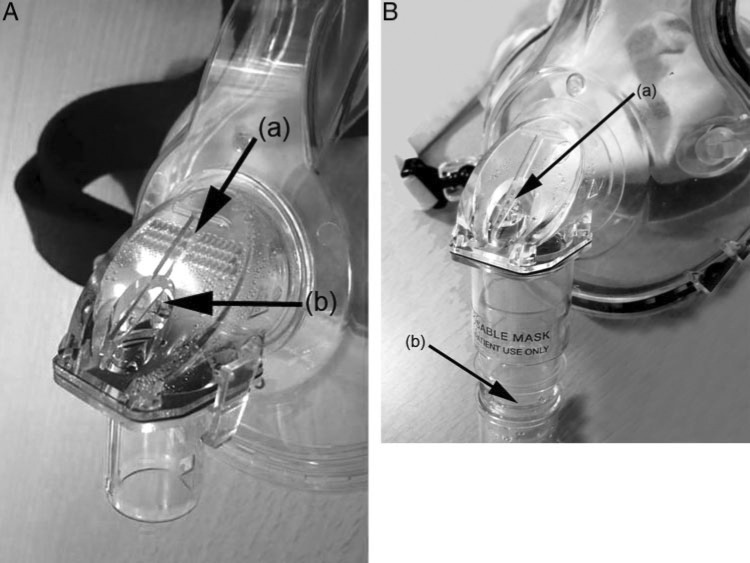
Background: As part of our influenza pandemic preparedness, we studied the exhaled air dispersion distances and directions through two different face masks (Respironics; Murrysville, PA) attached to a human-patient simulator (HPS) during noninvasive positive-pressure ventilation (NPPV) in an isolation room with pressure of -5 Pa.
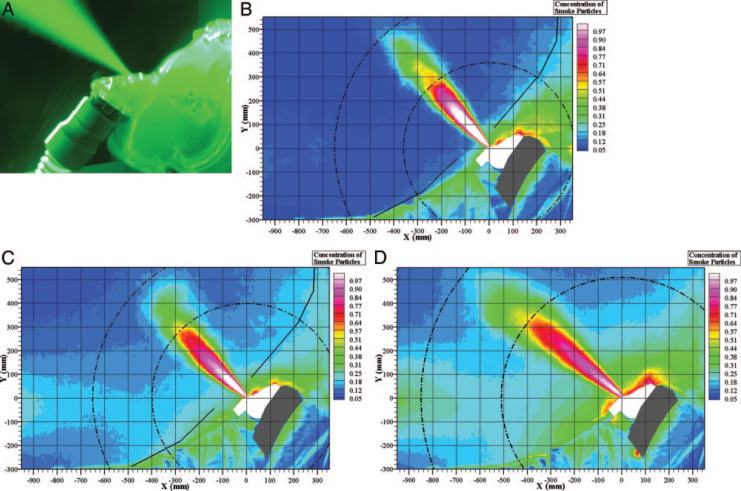
Methods: The HPS was positioned at 45 degrees on the bed and programmed to mimic mild lung injury (oxygen consumption, 300 mL/min; lung compliance, 35 mL/cm H(2)O). Airflow was marked with intrapulmonary smoke for visualization. Inspiratory positive airway pressure (IPAP) started at 10 cm H(2)O and gradually increased to 18 cm H(2)O, whereas expiratory pressure was maintained at 4 cm H(2)O. A leakage jet plume was revealed by a laser light sheet, and images were captured by high definition video. Normalized exhaled air concentration in the plume was estimated from the light scattered by the smoke particles.
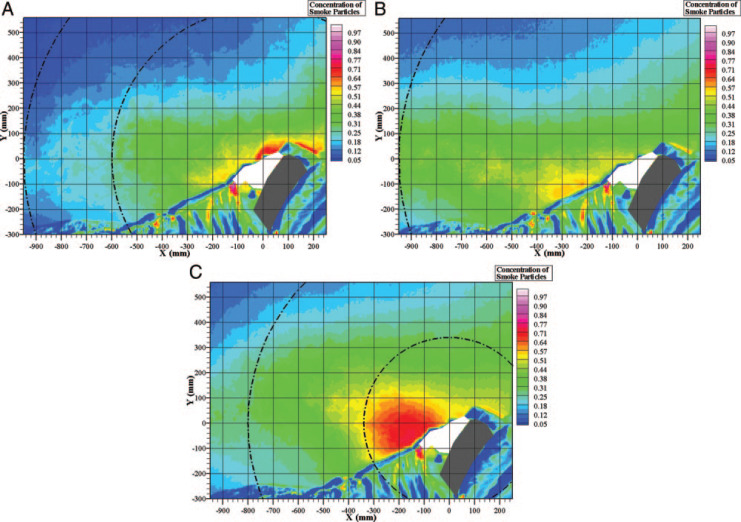
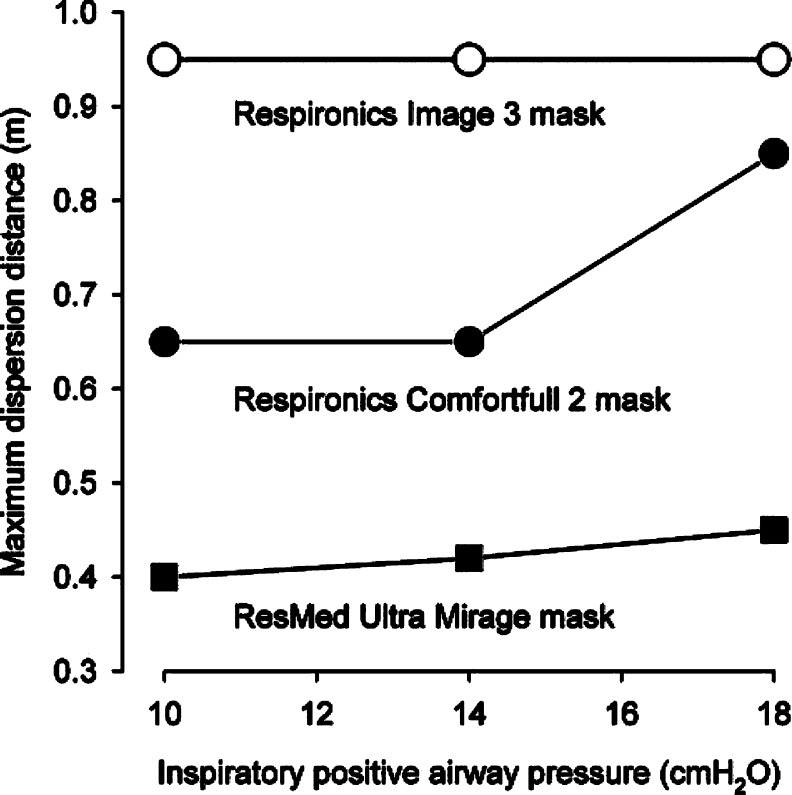
Findings: As IPAP increased from 10 to 18 cm H(2)O, the exhaled air of a low normalized concentration through the ComfortFull 2 mask (Respironics) increased from 0.65 to 0.85 m at a direction perpendicular to the head of the HPS along the median sagittal plane. When the IPAP of 10 cm H(2)O was applied via the Image 3 mask (Respironics) connected to the whisper swivel, the exhaled air dispersed to 0.95 m toward the end of the bed along the median sagittal plane, whereas higher IPAP resulted in wider spread of a higher concentration of smoke.
Conclusions: Substantial exposure to exhaled air occurs within a 1-m region, from patients receiving NPPV via the ComfortFull 2 mask and the Image 3 mask, with more diffuse leakage from the latter, especially at higher IPAP.
Figures
Comment in
-
Keeping the workplace safe in troubled times.Chest. 2009 Oct;136(4):956-957. doi: 10.1378/chest.09-1132. Chest. 2009. PMID: 19809040 Free PMC article. No abstract available.
References
-
- Yuen KY, Chan PK, Peiris M. Clinical features and rapid viral diagnosis of human disease associated with avian influenza A H5N1 virus. Lancet. 1998;351:467–471. - PubMed
-
- Abdel-Ghafar AN, Chotpitayasunondh T, Gao Z. Writing committee of the second World Health Organization consultation on clinical aspects of human infection with avian influenza A (H5N1) virus: update on avian influenza A (H5N1) virus infection in humans. N Engl J Med. 2008;358:261–273. - PubMed
-
- Arabi Y, Gomersall CD, Ahmed QA. The critically ill avian influenza A (H5N1) patient. Crit Care Med. 2007;35:1397–1403. - PubMed
-
- Hui DS. Review of clinical symptoms and spectrum in humans with influenza A/H5N1 infection. Respirology. 2008;13(suppl):S10–S13. - PubMed
-
- Hui DS. Influenza A/H5N1 infection: other treatment options and issues. Respirology. 2008;13(suppl):S22–S26. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
