

The silent estrogen receptor--can we make it speak?
- PMID: 19411863
- PMCID: PMC3901993
- DOI: 10.4161/cbt.8.6.7582
The silent estrogen receptor--can we make it speak?
Abstract
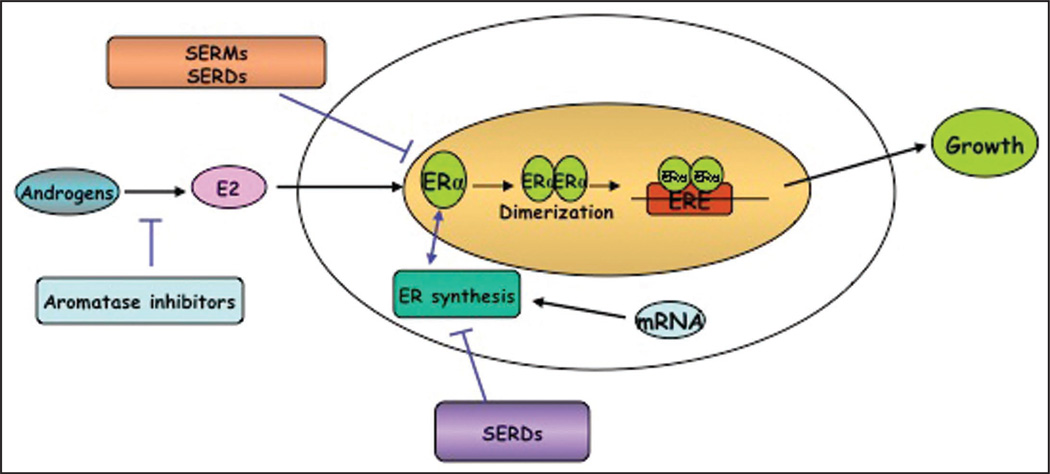
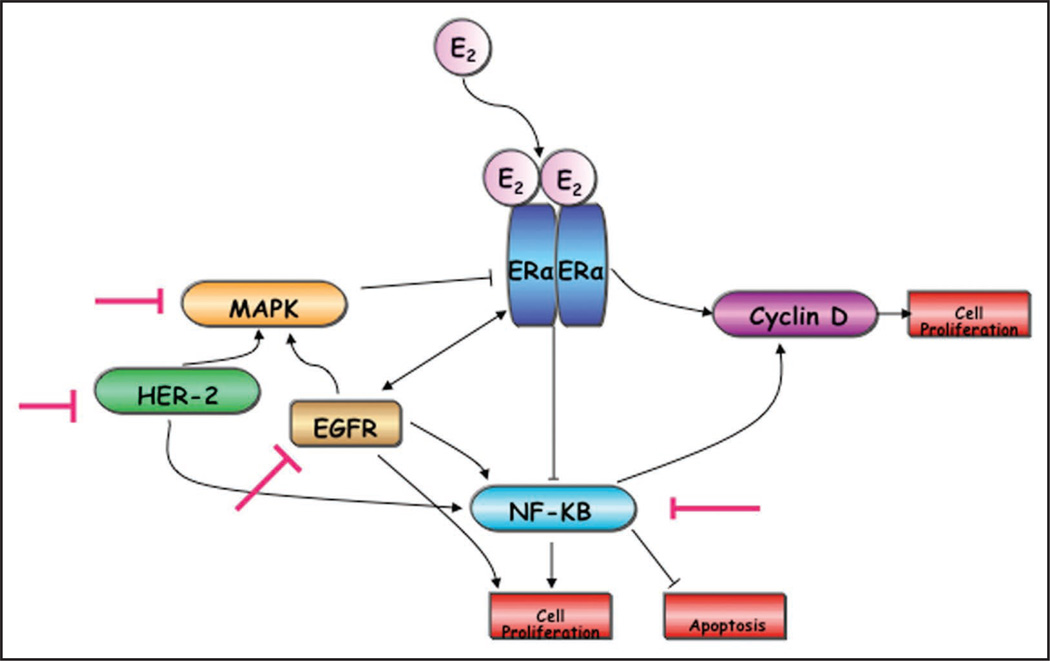
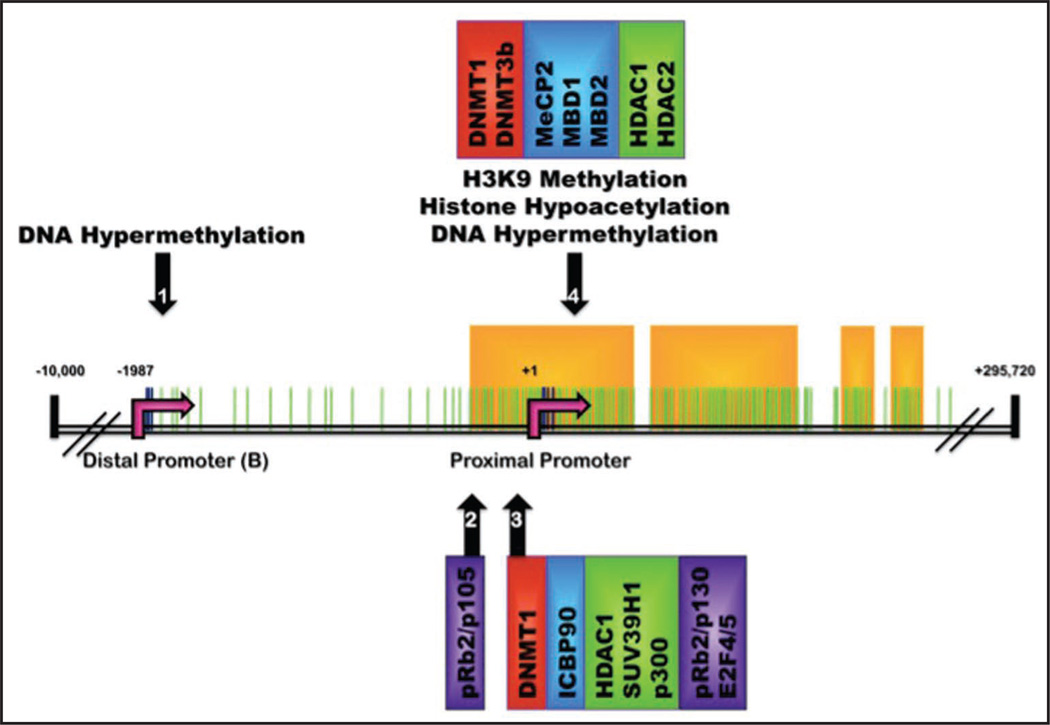
One of the most common cancers in women world wide, breast cancer is classically an endocrine-dependent cancer. It has been known for over a century that development, progression and metastasis of breast cancer are strongly influenced by hormonal factors. Indeed about two-thirds of breast cancers express the estrogen receptor α (ERα) protein, a key predictor of prognosis and response to endocrine therapy. These cancers are frequently amenable to therapies that target estrogen signaling pathways, including selective estrogen receptor modulators like tamoxifen, selective estrogen receptor downregulators like fulvestrant; and agents that reduce estrogen ligand like aromatase inhibitors and ovarian suppression through luteinizing hormone-releasing hormone (LHRH) agonists. It is likely that these approaches, especially adjuvant tamoxifen, have contributed to the reduction in breast cancer mortality that has been observed in recent years. However, data from clinical studies have suggested that only about 60% of ERα-positive breast cancers respond to hormonal therapy. Further, those tumors that lack expression of ERα and the estrogen-regulated progesterone receptor (PgR) are unresponsive to hormone therapy. Thus the problem of acquired or de novo endocrine resistance is a substantial one. Recent molecular and biological advances have contributed to our understanding about potential underlying mechanisms. Here we will focus especially on silencing the expression of ERα as one such endocrine-resistance mechanism and how it might be exploited clinically.
Figures
References
-
- ACS. Cancer Facts & Figures. Atlanta: American Cancer Society; 2008. 2008.
-
- Yager JD, Davidson NE. Estrogen carcinogenesis in breast cancer. N Engl J Med. 2006;354:270–282. - PubMed
-
- Effects of chemotherapy and hormonal therapy for early breast cancer on recurrence and 15-year survival: an overview of the randomised trials. Lancet. 2005;365:1687–1717. - PubMed
-
- McGuire WL. Hormone receptors: their role in predicting prognosis and response to endocrine therapy. Semin Oncol. 1978;5:428–433. - PubMed
-
- McGuire WL, Horwitz KB, Zava DT, Garola RE, Chamness GC. Hormones in breast cancer: update 1978. Metabolism. 1978;27:487–501. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials