

Mutational analysis of glycyl-tRNA synthetase (GARS) gene in Hirayama disease
- PMID: 19412816
- PMCID: PMC2864347
- DOI: 10.3109/17482960902849823
Mutational analysis of glycyl-tRNA synthetase (GARS) gene in Hirayama disease
Abstract
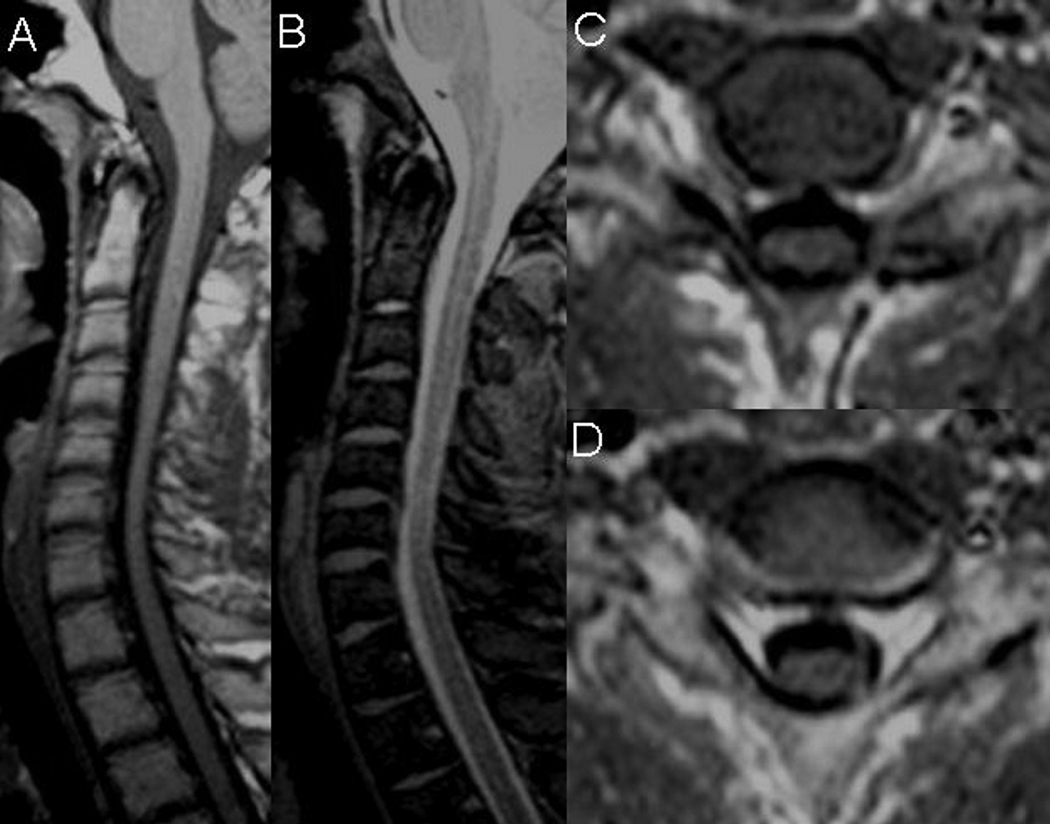
Sporadic juvenile muscular atrophy of the distal upper extremity or Hirayama's disease (HD) and autosomal dominant motor distal neuronopathy/axonopathy (CMT2D/dSMA-V), produced by glycyl-tRNA synthetase (GARS) gene mutations, share some clinical features including: young age of onset, predilection for the distal upper extremity, asymmetry, sparing of proximal muscles and unusual cold sensitivity. However, incomplete penetrance of GARS gene mutations may account for apparently non-familial cases. In order to inquire whether GARS gene mutations are associated with HD we studied seven patients fulfilling the clinical and electrodiagnostic criteria for HD. All patients underwent MRI of cervical spine that excluded compressive myelopathy in neutral position and intramedullary pathology. Each patient was tested for the presence of mutations in GARS by sequencing all coding exons amplified from genomic DNA. No pathogenic mutations were found, excluding the role of GARS gene as a possible factor in the aetiology of HD in this cohort.
Figures
References
-
- Hirayama K, Tokumaru Y. Cervical dural sac and spinal cord in juvenile muscular atrophy of distal upper extremity. Neurology. 2000;54:1922–1926. - PubMed
-
- Misra UK, Kalita J, Mishra VN, Kesari A, Mittal B. A clinical, magnetic resonance imaging and survival motor neuron gene deletion study of Hirayama Disease. Arch Neurol. 2005;62:120–123. - PubMed
-
- Fu I, Pei X, Zhang J, Kang D, Han H, Fan D. Morphological changes of the lower cervical spinal cord under neutral and fully flexed position by MRI in Chinese patients with Hirayama's disease. Amyotroph Lateral Scler. 2008;9:156–162. - PubMed
-
- Schroder R, Keller E, Flacke S, Schmidt S, Pohl C, Klockgether T, Schlegel R. MRI findings in Hirayama's disease: flexion-induced cervical myelopathy or intrinsic motor neuron disease ? J Neurol. 1999;246:1069–1074. - PubMed
-
- Willeit J, Kiechl S, Kiechl-Kohlendorfer U, Golaszewski S, Peer S, Poewe W. Juvenile asymmetric segmental spinal muscular atrophy (Hirayama's disease) Three cases without evidence of "flexion myelopathy". Acta Neurol Scand. 2008;104(5):320–322. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical