

High-resolution manometry in clinical practice: utilizing pressure topography to classify oesophageal motility abnormalities
- PMID: 19413684
- PMCID: PMC2892003
- DOI: 10.1111/j.1365-2982.2009.01311.x
High-resolution manometry in clinical practice: utilizing pressure topography to classify oesophageal motility abnormalities
Abstract
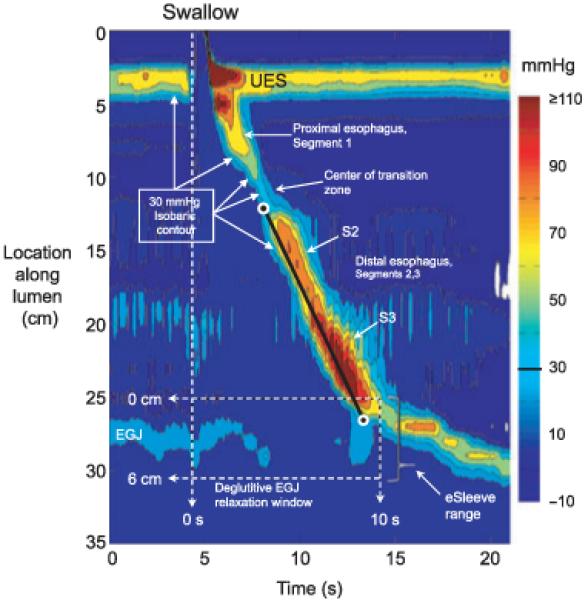
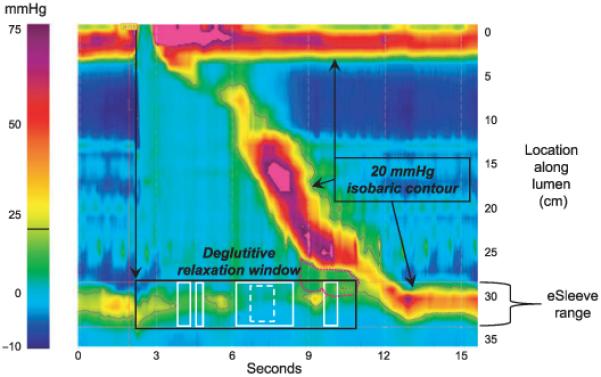
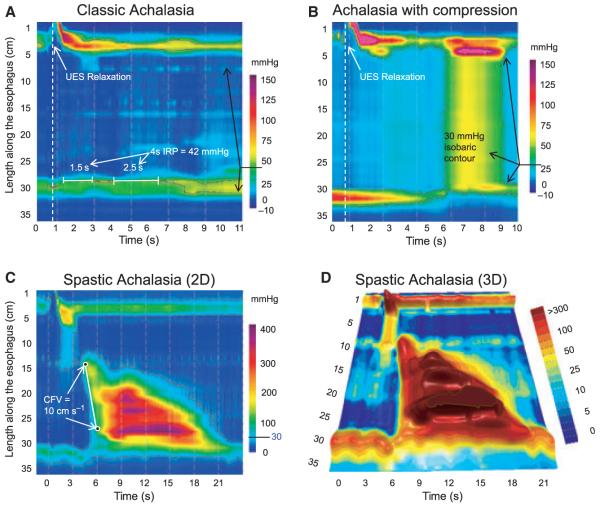
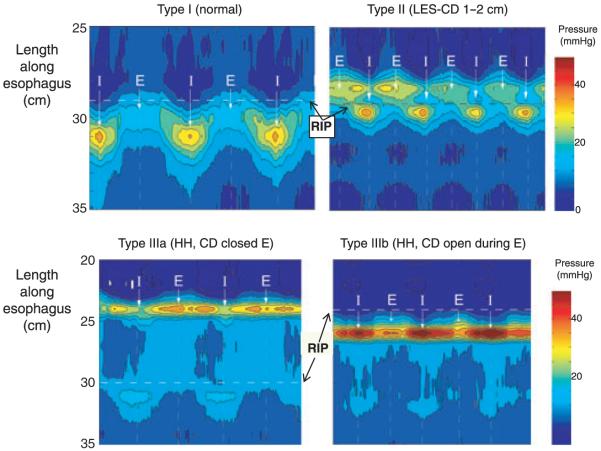
High-resolution manometry capable of pressure monitoring from the pharynx to the stomach together with pressure topography plotting represents an unquestionable evolution in oesophageal manometry. However, with this advanced technology come challenges and one of those is devising the optimal scheme to apply high-resolution oesophageal pressure topography (HROPT) to the clinical evaluation of patients. The first iteration of the Chicago classification was based on a systematic analysis of motility patterns in 75 control subjects and 400 consecutive patients. This review summarizes the analysis process as it has evolved. Individual swallows are analysed in a stepwise fashion for the morphology of the oesophagogastric junction (OGJ), the extent of OGJ relaxation, the propagation velocity of peristalsis, the vigour of the peristaltic contraction, and abnormalities of intrabolus pressure utilizing metrics that have now been customized to HROPT. These results are then synthesized into a comprehensive diagnosis that, although based on conventional manometry criteria, is also customized to HROPT measures. The resultant classification objectifies the identification of three unique subtypes of achalasia. Additionally, it provides enhanced detail in the description of distal oesophageal spasm, nutcracker oesophagus subtypes, and OGJ obstruction. It is our expectation that modification of this classification scheme will continue to occur and this should further clarify the utility of pressure topography plotting in assessing oesophageal motility disorders.
Figures
References
-
- Clouse RE, Staiano A. Topography of the esophageal peristaltic pressure wave. Am J Physiol. 1991;261:G677–84. - PubMed
-
- Grubel C, Hiscock R, Hebbard G. Value of spatiotemporal representation of manometric data. Clin Gastroenterol Hepatol. 2008;6:525–30. - PubMed
-
- Pandolfino JE, Ghosh SK, Zhang Q, Jarosz A, Shah N, Kahrilas PJ. Quantifying OGJ morphology and relaxation with high-resolution manometry: a study of 75 asymptomatic volunteers. Am J Physiol Gastrointest Liver Physiol. 2006;290:G988–97. - PubMed
-
- Ghosh SK, Pandolfino JE, Zhang Q, Jarosz A, Shah N, Kahrilas PJ. Quantifying esophageal peristalsis with high-resolution manometry: a study of 75 asymptomatic volunteers. Am J Physiol Gastrointest Liver Physiol. 2006;290:G988–97. - PubMed
-
- Ghosh SK, Pandolfino JE, Rice J, Clarke JO, Kwiatek M, Kahrilas PJ. Impaired deglutitive OGJ relaxation in clinical esophageal manometry: a quantitative analysis of 400 patients and 75 controls. Am J Physiol Gastrointest Liver Physiol. 2007;293:G878–85. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
