

Case Reports
doi: 10.1002/pbc.22067.
Heparin induced thrombocytopenia and re-thrombosis associated with warfarin and fondaparinux in a child
Affiliations
- PMID: 19415734
- PMCID: PMC4778081
- DOI: 10.1002/pbc.22067
Item in Clipboard
Case Reports
Heparin induced thrombocytopenia and re-thrombosis associated with warfarin and fondaparinux in a child
Pediatr Blood Cancer.
2009 Sep.
Abstract
An 11-year-old female developed heparin induced thrombocytopenia (HIT) with thrombosis during therapy for lower extremity deep vein thrombosis and pulmonary embolism. Transition from bivalirudin, a direct thrombin inhibitor (DTI), to warfarin resulted in extensive re-thrombosis, and fondaparinux therapy similarly failed. She was then treated with argatroban, and transitioned successfully to warfarin after 9 weeks. The risk of re-thrombosis was ultimately reduced by allowing time for the thrombogenic potential to abate. The argatroban/warfarin transition was monitored with chromogenic factor X levels. This case highlights several difficult problems in pediatric thrombosis.
(c) 2009 Wiley-Liss, Inc.
Figures
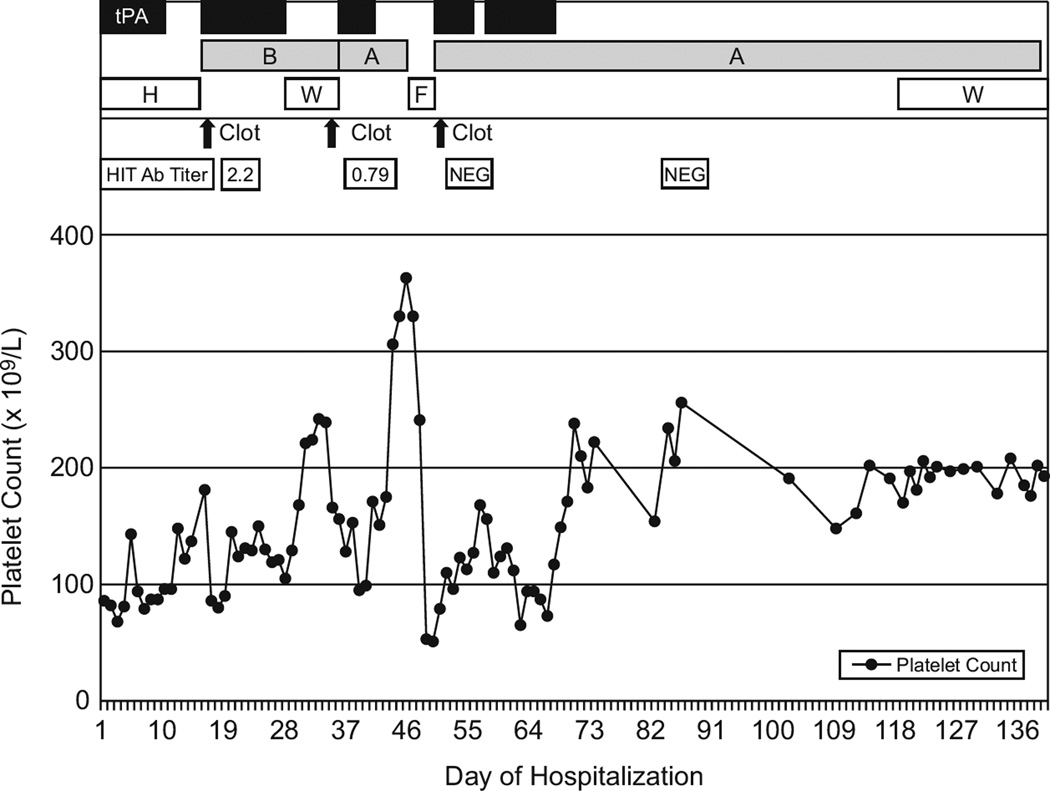
Course of the patient’s platelet count, thrombotic events, anti-heparin:PF4 antibody titer (HIT Ab titer), and therapy. tPA, tissue plasminogen activator; B, bivalirudin; A, argatroban; H, heparin/low molecular weight heparin; W, warfarin; F, fondaparinux; NEG, negative.
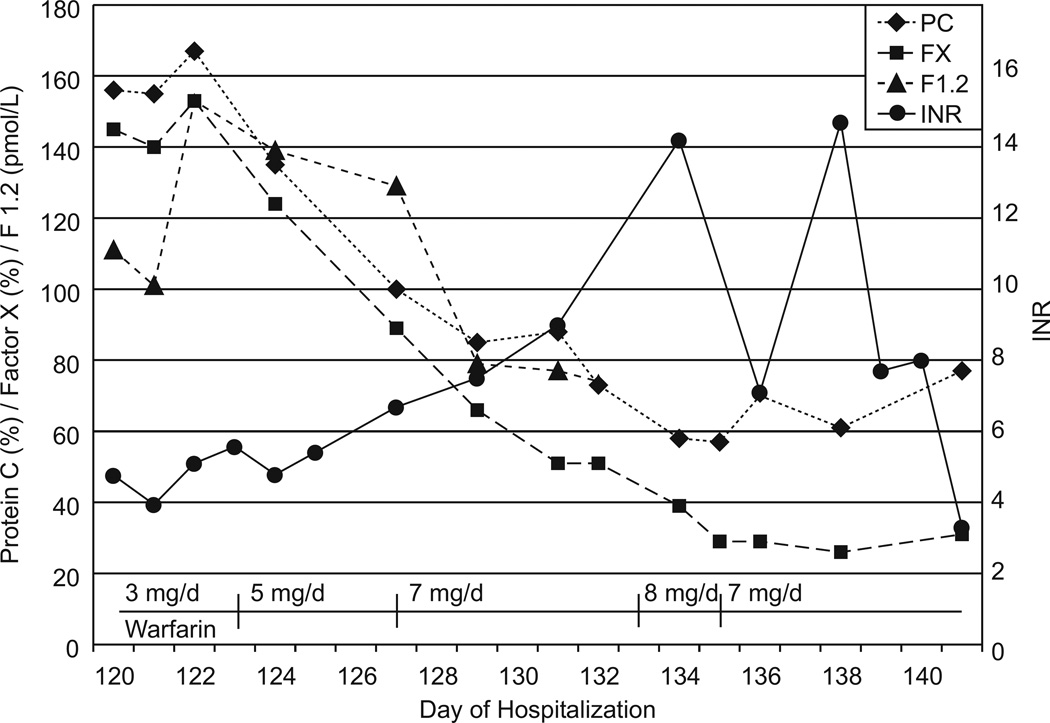
Changes in protein C activity (PC), chromogenic factor X level (FX), prothrombin fragment 1.2 (F1.2), INR, and warfarin dose changes during the transition from argatroban to warfarin. D-dimer is not shown but started at 0.81 FEU/mL (normal <0.36) and consistently decreased to 0.28 FEU/mL (normal <0.45) over this time period.
References
-
- Dager WE, Dougherty JA, Nguyen PH, et al. Heparin-Induced Thrombocytopenia: Treatment Options and Special Considerations. Pharmacotherapy. 2007;27:564–587. - PubMed
-
- Prechel M, Walenga JM. The Laboratory Diagnosis and Clinical Management of Patients with Heparin-Induced Thrombocytopenia: An Update. Semin Thromb Haemost. 2008;34:86–96. - PubMed
-
- Greinacher A, Warkentin TE. Recognition, Treatment, and Prevention of Heparin-Induced Thrombocytopenia: Review and Update. Thromb Res. 2006;118:165–176. - PubMed
-
- Klenner AF, Lubenow N, Raschke R, Greinacher A. Heparin-Induced Thrombocytopenia in Children: 12 New Cases and Review of the Literature. Thromb Haemost. 2004;91:719–724. - PubMed
-
- Warkentin TE. Heparin-Induced Thrombocytopenia: Pathogenesis and Management. Br J Haematol. 2003;121:535–555. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
