

The public health approach to identify antiretroviral therapy failure: high-level nucleoside reverse transcriptase inhibitor resistance among Malawians failing first-line antiretroviral therapy
- PMID: 19417582
- PMCID: PMC2896488
- DOI: 10.1097/QAD.0b013e32832ac34e
The public health approach to identify antiretroviral therapy failure: high-level nucleoside reverse transcriptase inhibitor resistance among Malawians failing first-line antiretroviral therapy
Abstract
Background: Over 150,000 Malawians have started antiretroviral therapy (ART), in which first-line therapy is stavudine/lamivudine/nevirapine. We evaluated drug resistance patterns among patients failing first-line ART on the basis of clinical or immunological criteria in Lilongwe and Blantyre, Malawi.
Methods: Patients meeting the definition of ART failure (new or progressive stage 4 condition, CD4 cell count decline more than 30%, CD4 cell count less than that before treatment) from January 2006 to July 2007 were evaluated. Among those with HIV RNA of more than 1000 copies/ml, genotyping was performed. For complex genotype patterns, phenotyping was performed.
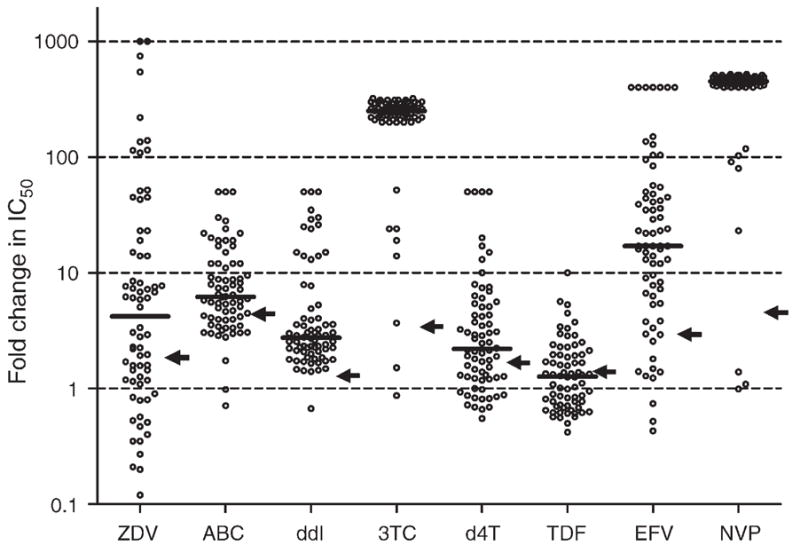
Results: Ninety-six confirmed ART failure patients were identified. Median (interquartile range) CD4 cell count, log10 HIV-1 RNA, and duration on ART were 68 cells/microl (23-174), 4.72 copies/ml (4.26-5.16), and 36.5 months (26.6-49.8), respectively. Ninety-three percent of samples had nonnucleoside reverse transcriptase inhibitor mutations, and 81% had the M184V mutation. The most frequent pattern included M184V and nonnucleoside reverse transcriptase inhibitor mutations along with at least one thymidine analog mutation (56%). Twenty-three percent of patients acquired the K70E or K65R mutations associated with tenofovir resistance; 17% of the patients had pan-nucleoside resistance that corresponded to K65R or K70E and additional resistance mutations, most commonly the 151 complex. Emergence of the K65R and K70E mutations was associated with CD4 cell count of less than 100 cells/microl (odds ratio 6.1) and inversely with the use of zidovudine (odds ratio 0.18). Phenotypic susceptibility data indicated that the nucleoside reverse transcriptase inhibitor backbone with the highest activity for subsequent therapy was zidovudine/lamivudine/tenofovir, followed by lamivudine/tenofovir, and then abacavir/didanosine.
Conclusion: When clinical and CD4 cell count criteria are used to monitor first-line ART failure, extensive nucleoside reverse transcriptase inhibitor and nonnucleoside reverse transcriptase inhibitor resistance emerges, with most patients having resistance profiles that markedly compromise the activity of second-line ART.
Figures
References
-
- Harries AD, Schouten EJ, Libamba E. Scaling up antiretroviral treatment in resource-poor settings. Lancet. 2006;367:1870–1872. - PubMed
-
- HIV Unit. ART quarterly report for December 2007. Ministry of Health; Malawi: 2007.
-
- National AIDS Commission and Malawi Ministry of Health and Population. Treatment of AIDS: guidelines for the use of antiretroviral therapy in Malawi. 2. Apr2006. [Accessed January 2009]. http://www.hivunitmohmw.org/Main/AntiretroviralTherapy.
-
- WHO. Recommendations for a public health approach. 2006. Geneva: WHO; 2006. Antiretroviral therapy for HIV infection in adults and adolescents in resource-limited settings: toward universal access.
-
- WHO. Report of a WHO Working Group Meeting. Geneva: WHO; 2007. Prioritizing second line antiretroviral drugs for adults and adolescents: a public health approach.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
