

Total pelvic exenteration for primary and recurrent malignancies
- PMID: 19421811
- PMCID: PMC2691931
- DOI: 10.1007/s00268-009-0066-7
Total pelvic exenteration for primary and recurrent malignancies
Abstract
Introduction: Complete resection is the most important prognostic factor in surgery for pelvic tumors. In locally advanced and recurrent pelvic malignancies, radical margins are sometimes difficult to obtain because of close relation to or growth in adjacent organs/structures. Total pelvic exenteration (TPE) is an exenterative operation for these advanced tumors and involves en bloc resection of the rectum, bladder, and internal genital organs (prostate/seminal vesicles or uterus, ovaries and/or vagina).
Methods: Between 1994 and 2008, a TPE was performed in 69 patients with pelvic cancer; 48 with rectal cancer (32 primary and 16 recurrent), 14 with cervical cancer (1 primary and 13 recurrent), 5 with sarcoma (3 primary and 2 recurrent), 1 with primary vaginal, and 1 with recurrent endometrial carcinoma. Ten patients were treated with neoadjuvant chemotherapy and 66 patients with preoperative radiotherapy to induce down-staging. Eighteen patients received IORT because of an incomplete or marginal complete resection.
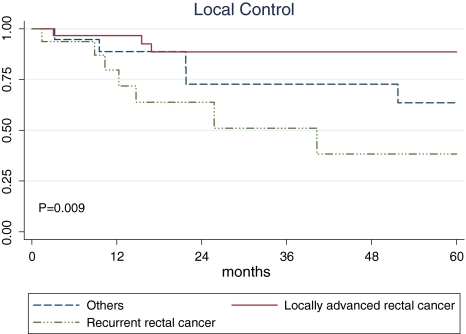
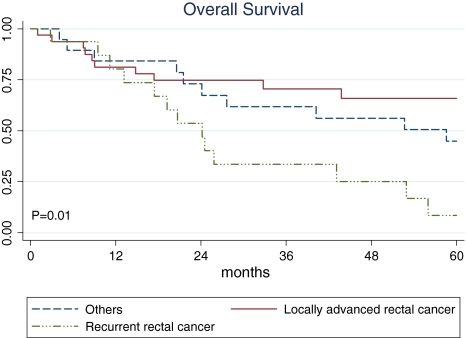
Results: The median follow-up was 43 (range, 1-196) months. Median duration of surgery was 448 (range, 300-670) minutes, median blood loss was 6,300 (range, 750-21,000) ml, and hospitalization was 17 (range, 4-65) days. Overall major and minor complication rates were 34% and 57%, respectively. The in-hospital mortality rate was 1%. A complete resection was possible in 75% of all patients, a microscopically incomplete resection (R1) in 16%, and a macroscopically incomplete resection (R2) in 9%. Five-year local control for primary locally advanced rectal cancer, recurrent rectal cancer, and cervical cancer was 89%, 38%, and 64%, respectively. Overall survival after 5 years for primary locally advanced rectal cancer, recurrent rectal cancer, and cervical cancer was 66%, 8%, and 45%.
Conclusions: Total pelvic exenteration is accompanied with considerable morbidity, but good local control and acceptable overall survival justifies the use of this extensive surgical technique in most patients, especially patients with primary locally advanced rectal cancer and recurrent cervical cancer.
Figures
References
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1007/s10350-006-0651-x', 'is_inner': False, 'url': 'https://doi.org/10.1007/s10350-006-0651-x'}, {'type': 'PubMed', 'value': '16912909', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/16912909/'}]}
- Ferenschild FT, Vermaas M, Nuyttens JJ et al (2006) Value of intraoperative radiotherapy in locally advanced rectal cancer. Dis Colon Rectum 49:1257–1265 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1007/s10350-004-0891-6', 'is_inner': False, 'url': 'https://doi.org/10.1007/s10350-004-0891-6'}, {'type': 'PubMed', 'value': '15785886', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/15785886/'}]}
- Vermaas M, Ferenschild FT, Nuyttens JJ et al (2005) Preoperative radiotherapy improves outcome in recurrent rectal cancer. Dis Colon Rectum 48:918–928 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.ejso.2006.09.021', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.ejso.2006.09.021'}, {'type': 'PubMed', 'value': '17071043', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/17071043/'}]}
- Vermaas M, Ferenschild FT, Verhoef C et al (2007) Total pelvic exenteration for primary locally advanced and locally recurrent rectal cancer. Eur J Surg Oncol 33:452–458 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'PubMed', 'value': '14782163', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/14782163/'}]}
- Bricker EM (1950) Bladder substitution after pelvic evisceration. Surg Clin N Am 30:1511 - PubMed
-
- {'text': '', 'ref_index': 1, 'ids': [{'type': 'DOI', 'value': '10.1016/j.ejso.2003.08.008', 'is_inner': False, 'url': 'https://doi.org/10.1016/j.ejso.2003.08.008'}, {'type': 'PubMed', 'value': '14602493', 'is_inner': True, 'url': 'https://pubmed.ncbi.nlm.nih.gov/14602493/'}]}
- Kecmanovic DM, Pavlov MJ, Kovacevic PA, Sepetkovski AV, Ceranic MS, Stamenkovic AB (2003) Management of advanced pelvic cancer by exenteration. Eur J Surg Oncol 29:743–746 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
