

Case mix, quality and high-cost kidney transplant patients
- PMID: 19422336
- PMCID: PMC2857520
- DOI: 10.1111/j.1600-6143.2009.02592.x
Case mix, quality and high-cost kidney transplant patients
Abstract
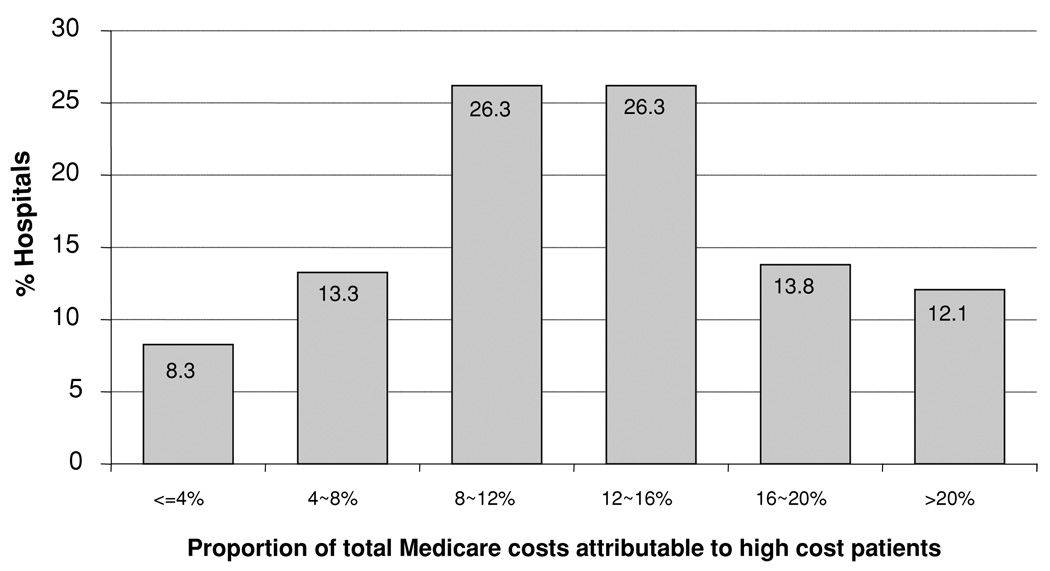
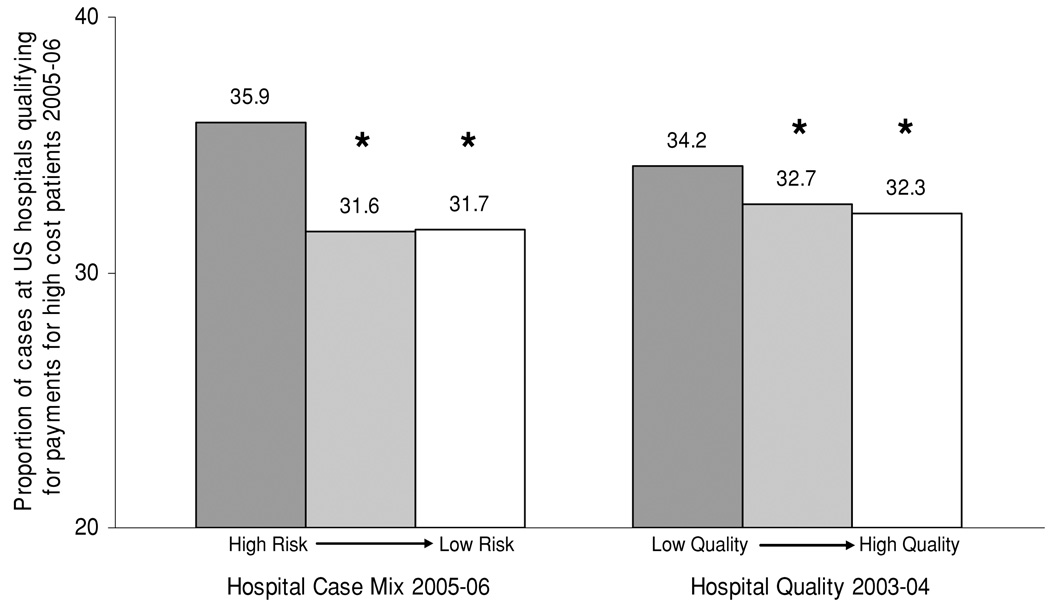
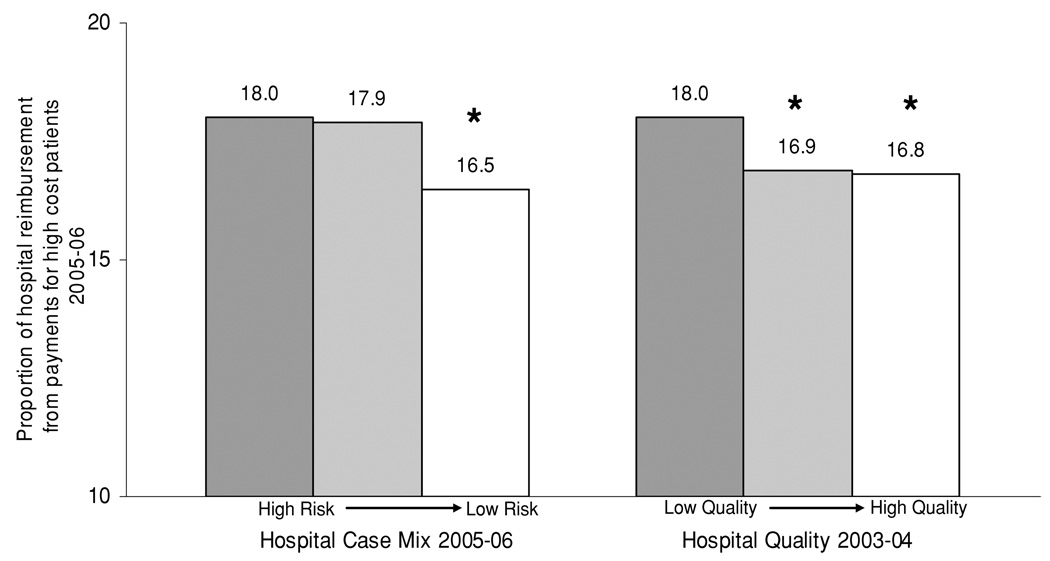
A better understanding of high-cost kidney transplant patients would be useful for informing value-based purchasing strategies by payers. This retrospective cohort study was based on the Medicare Provider Analysis and Review (MEDPAR) files from 2003 to 2006. The focus of this analysis was high-cost kidney transplant patients (patients that qualified for Medicare outlier payments and 30-day readmission payments). Using regression techniques, we explored relationships between high-cost kidney transplant patients, center-specific case mix, and center quality. Among 43 393 kidney transplants in Medicare recipients, 35.2% were categorized as high-cost patients. These payments represented 20% of total Medicare payments for kidney transplantation and exceeded $200 million over the study period. Case mix was associated with these payments and was an important factor underlying variation in hospital payments high-cost patients. Hospital quality was also a strong determinant of future Medicare payments for high-cost patients. Compared to high-quality centers, low-quality centers cost Medicare an additional $1185 per kidney transplant. Payments for high-cost patients represent a significant proportion of the total costs of kidney transplant surgical care. Quality improvement may be an important strategy for reducing the costs of kidney transplantation.
Figures
Comment in
-
The cost and quality paradox.Am J Transplant. 2009 May;9(5):985-6. doi: 10.1111/j.1600-6143.2009.02600.x. Am J Transplant. 2009. PMID: 19422326 No abstract available.
References
-
- Englesbe MJ, Dubay DA, Gillespie BW, et al. Risk factors for urinary complications after renal transplantation. Am J Transplant. 2007;7:1536–1541. - PubMed
-
- DuBay DA, Lynch R, Cohn J, et al. Is routine ureteral stenting cost-effective in renal transplantation? J Urol. 2007;178:2509–2513. discussion 13. - PubMed
-
- The USRDS 2006 Annual Report. [Accessed March 26, 2009]. Available from: www.usrds.org.
-
- World Health Organization (WHO) World Health Statistics. 2005. [Accessed March 26, 2009]. Available from: http://www.who.int/healthinfo/statistics/en/.
-
- Dimick JB, Chen SL, Taheri PA, Henderson WG, Khuri SF, Camp-bell DA., Jr Hospital costs associated with surgical complications: A report from the private-sector National Surgical Quality Improvement Program. J Am Coll Surg. 2004;199:531–537. - PubMed
