

Targeted endoscopic imaging
- PMID: 19423025
- PMCID: PMC3217463
- DOI: 10.1016/j.giec.2009.02.001
Targeted endoscopic imaging
Abstract
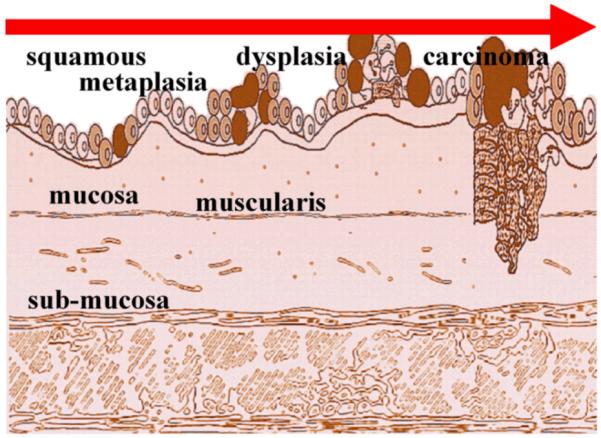
Endoscopy has undergone explosive technological growth in recent years, and with the emergence of targeted imaging, its truly transformative power and impact on medicine lies just over the horizon. Today, our ability to see inside the digestive tract with medical endoscopy is headed toward exciting crossroads. The existing paradigm of making diagnostic decisions based on observing structural changes and identifying anatomic landmarks may soon be replaced by visualizing functional properties and imaging molecular expression. In this novel approach, the presence of intracellular and cell surface targets unique to disease are identified and used to predict the likelihood of mucosal transformation and response to therapy. This strategy could result in the development of new methods for early cancer detection, personalized therapy, and chemoprevention. This targeted approach will require further development of molecular probes and endoscopic instruments, and will need support from the US Food and Drug Administration for streamlined regulatory oversight. Overall, this molecular imaging modality promises to significantly broaden the capabilities of the gastroenterologist by providing a new approach to visualize the mucosa of the digestive tract in a manner that has never been seen before.
Figures

Similar articles
-
Image-enhanced endoscopy technology in the gastrointestinal tract: what is available?Best Pract Res Clin Gastroenterol. 2015 Aug;29(4):627-38. doi: 10.1016/j.bpg.2015.05.008. Epub 2015 Jun 4. Best Pract Res Clin Gastroenterol. 2015. PMID: 26381307 Review.
-
New endoscopic and cytologic tools for cancer surveillance in the digestive tract.Gastrointest Endosc Clin N Am. 2009 Apr;19(2):299-307. doi: 10.1016/j.giec.2009.02.002. Gastrointest Endosc Clin N Am. 2009. PMID: 19423026 Free PMC article.
-
A guide to multimodal endoscopy imaging for gastrointestinal malignancy - an early indicator.Nat Rev Gastroenterol Hepatol. 2017 Jul;14(7):421-434. doi: 10.1038/nrgastro.2017.46. Epub 2017 Jun 14. Nat Rev Gastroenterol Hepatol. 2017. PMID: 28611477 Review.
-
Autofluorescence imaging and magnification endoscopy.World J Gastroenterol. 2011 Jan 7;17(1):9-14. doi: 10.3748/wjg.v17.i1.9. World J Gastroenterol. 2011. PMID: 21218078 Free PMC article.
-
Modern methods of endoscopic diagnosis of gastrointestinal tract.J Physiol Pharmacol. 2007 Aug;58 Suppl 3:21-31. J Physiol Pharmacol. 2007. PMID: 17901580 Review.
Cited by
-
Recent advances in targeted endoscopic imaging: Early detection of gastrointestinal neoplasms.World J Gastrointest Endosc. 2012 Mar 16;4(3):57-64. doi: 10.4253/wjge.v4.i3.57. World J Gastrointest Endosc. 2012. PMID: 22442742 Free PMC article.
-
Future and advances in endoscopy.J Biophotonics. 2011 Aug;4(7-8):471-81. doi: 10.1002/jbio.201100048. Epub 2011 Jul 13. J Biophotonics. 2011. PMID: 21751414 Free PMC article. Review.
-
Molecular imaging in gastrointestinal endoscopy.Gastroenterology. 2010 Mar;138(3):828-33.e1. doi: 10.1053/j.gastro.2010.01.009. Epub 2010 Jan 21. Gastroenterology. 2010. PMID: 20096697 Free PMC article. Review.
-
Multicolor fluorescence imaging using a single RGB-IR CMOS sensor for cancer detection with smURFP-labeled probiotics.Biomed Opt Express. 2020 May 8;11(6):2951-2963. doi: 10.1364/BOE.391417. eCollection 2020 Jun 1. Biomed Opt Express. 2020. PMID: 32637234 Free PMC article.
-
Molecular endoscopic imaging: the future is bright.Ther Adv Gastrointest Endosc. 2019 Sep 2;12:2631774519867175. doi: 10.1177/2631774519867175. eCollection 2019 Jan-Dec. Ther Adv Gastrointest Endosc. 2019. PMID: 31517311 Free PMC article. Review.
References
-
- Kumar V, Fausto N, Abbas A. Robbins & Cotran Pathologic Basis of Disease. 7th ed W. B. Saunders Company; Philadelphia: 2004.
-
- Levine DS, Haggitt RC, Blount PL, et al. An endoscopic biopsy protocol can differentiate high-grade dysplasia from early adenocarcinoma in Barrett’s esophagus. Gastroenterology. 1993;105(1):40–50. - PubMed
-
- Jess T, Loftus EV, Jr, Velayos FS, et al. Risk of intestinal cancer in inflammatory bowel disease: a population-based study from olmsted county, Minnesota. Gastroenterology. 2006;130(4):1039–46. - PubMed
-
- Vogelstein B, Kinzler KW. Cancer genes and the pathways they control. Nat Med. 2004;10(8):789–99. 21. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
