

Evaluation and management of priapism: 2009 update
- PMID: 19424174
- PMCID: PMC3905796
- DOI: 10.1038/nrurol.2009.50
Evaluation and management of priapism: 2009 update
Abstract
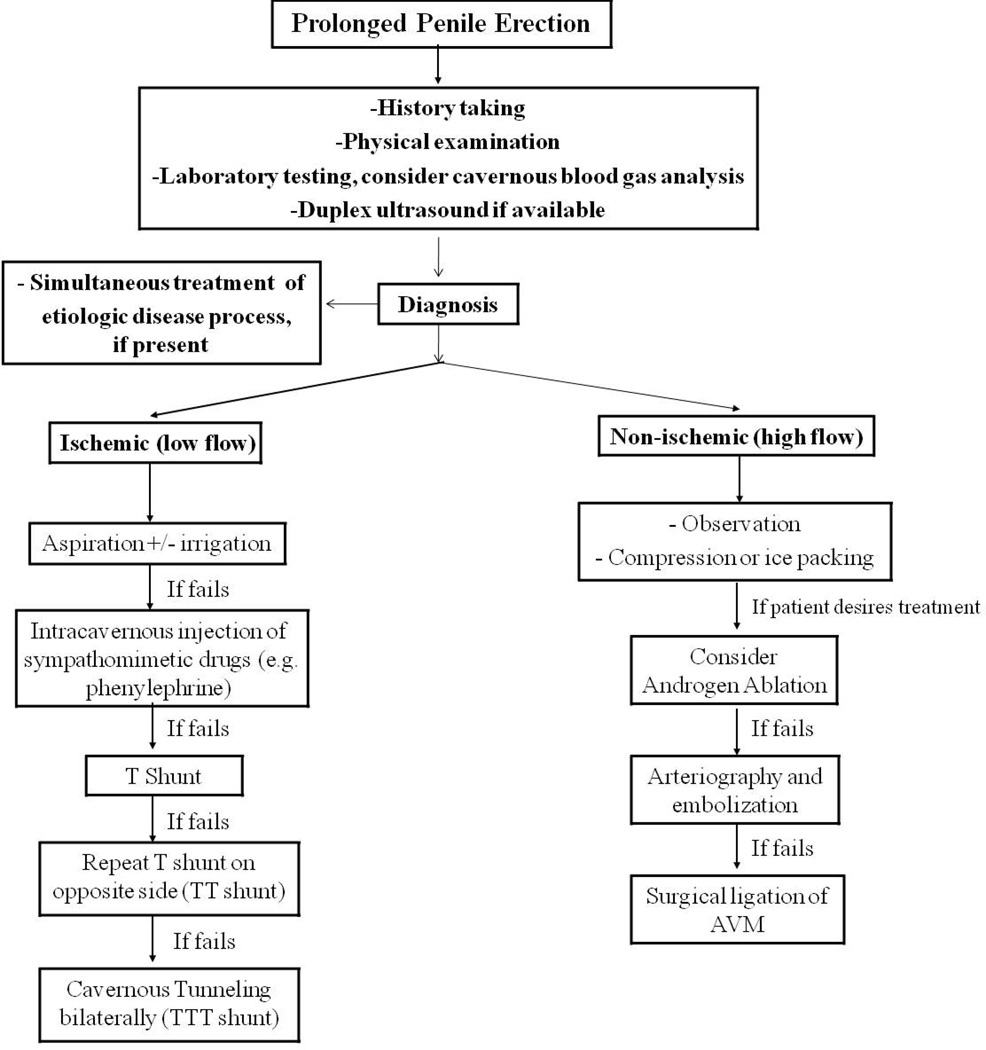
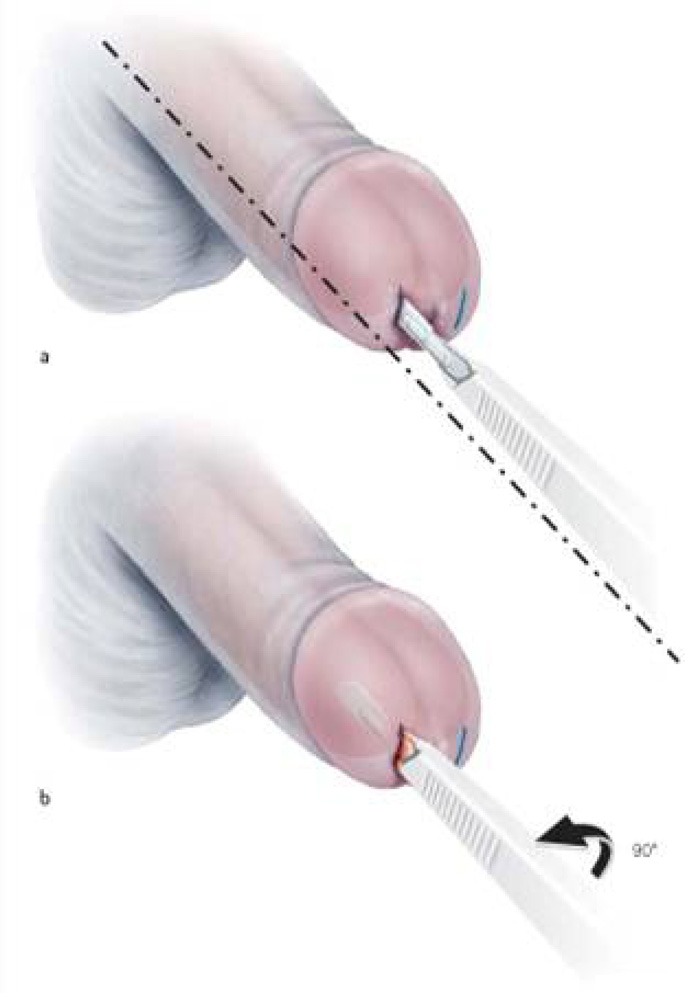
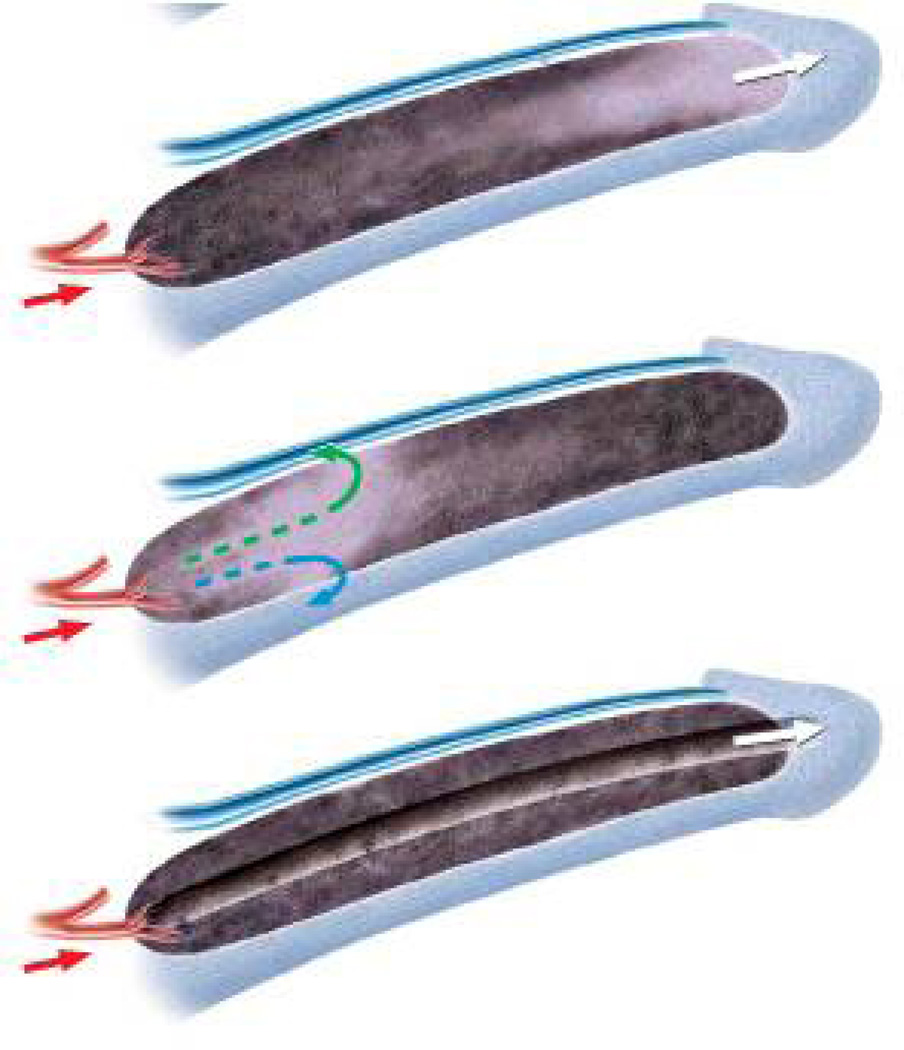
Priapism is defined as a persistent penile erection (typically 4 h or longer) that is unrelated to sexual stimulation. Priapism can be classified as either ischemic or nonischemic. Ischemic priapism, the most common subtype, is typically accompanied by pain and is associated with a substantial risk of subsequent erectile dysfunction. Prompt medical attention is indicated in cases of ischemic priapism. The initial management of choice is corporal aspiration with injection of sympathomimetic agents. If medical management fails, a cavernosal shunt procedure is indicated. Stuttering (recurrent) ischemic priapism is a challenging and poorly understood condition; new management strategies currently under investigation may improve our ability to care for men with this condition. Nonischemic priapism occurs more rarely than ischemic priapism, and is most often the result of trauma. This subtype of priapism, which is generally not painful, is usually initially managed with conservative treatment.
Figures


References
-
- Papadopoulos I, Kelami A. Priapus and priapism from mythology to medicine. Urology. 1988;32:385–386. - PubMed
-
- Montague DK, et al. American Urological Association guideline on the management of priapism. J Urol. 2003;70:1318–1324. - PubMed
-
- Eland, et al. Incidence of priapism in the general population. Urology. 2001;57:970–972. - PubMed
-
- Earle CM, et al. The incidence and management of priapism in Western Australia: a 16 year audit. Int J Impot Res. 2003;15:272–276. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
