

Intracerebral haemorrhage
- PMID: 19427958
- PMCID: PMC3138486
- DOI: 10.1016/S0140-6736(09)60371-8
Intracerebral haemorrhage
Abstract
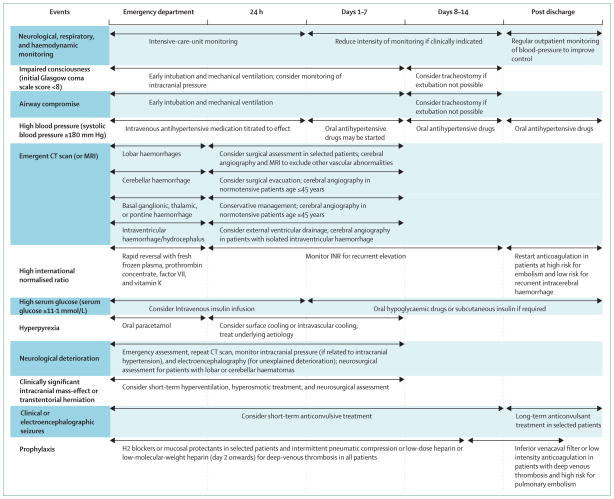
Intracerebral haemorrhage is an important public health problem leading to high rates of death and disability in adults. Although the number of hospital admissions for intracerebral haemorrhage has increased worldwide in the past 10 years, mortality has not fallen. Results of clinical trials and observational studies suggest that coordinated primary and specialty care is associated with lower mortality than is typical community practice. Development of treatment goals for critical care, and new sequences of care and specialty practice can improve outcome after intracerebral haemorrhage. Specific treatment approaches include early diagnosis and haemostasis, aggressive management of blood pressure, open surgical and minimally invasive surgical techniques to remove clot, techniques to remove intraventricular blood, and management of intracranial pressure. These approaches improve clinical management of patients with intracerebral haemorrhage and promise to reduce mortality and increase functional survival.
Figures
References
-
- Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, Hanley DF. Spontaneous intracerebral hemorrhage. N Engl J Med. 2001;344:1450–60. - PubMed
-
- Labovitz DL, Halim A, Boden-Albala B, Hauser WA, Sacco RL. The incidence of deep and lobar intracerebral hemorrhage in whites, blacks, and hispanics. Neurology. 2005;65:518–22. - PubMed
-
- Sudlow CL, Warlow CP. Comparable studies of the incidence of stroke and its pathological types: results from an international collaboration. Stroke. 1997;28:491–99. - PubMed
-
- American Heart Organization. [accessed Nov 21, 2007];International cardiovascular disease statistics: cardiovascular disease (CVD) http://www.americanheart.org/downloadable/heart/1140811583642Internation....
-
- Qureshi AI, Suri MFK, Nasar A, et al. Changes in cost and outcome among US patients with stroke hospitalized in 1990 to 1991 and those hospitalized in 2000 to 2001. Stroke. 2007;38:2180–84. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
