

Why prevent, diagnose and treat congenital toxoplasmosis?
- PMID: 19430661
- PMCID: PMC2735102
- DOI: 10.1590/s0074-02762009000200029
Why prevent, diagnose and treat congenital toxoplasmosis?
Abstract
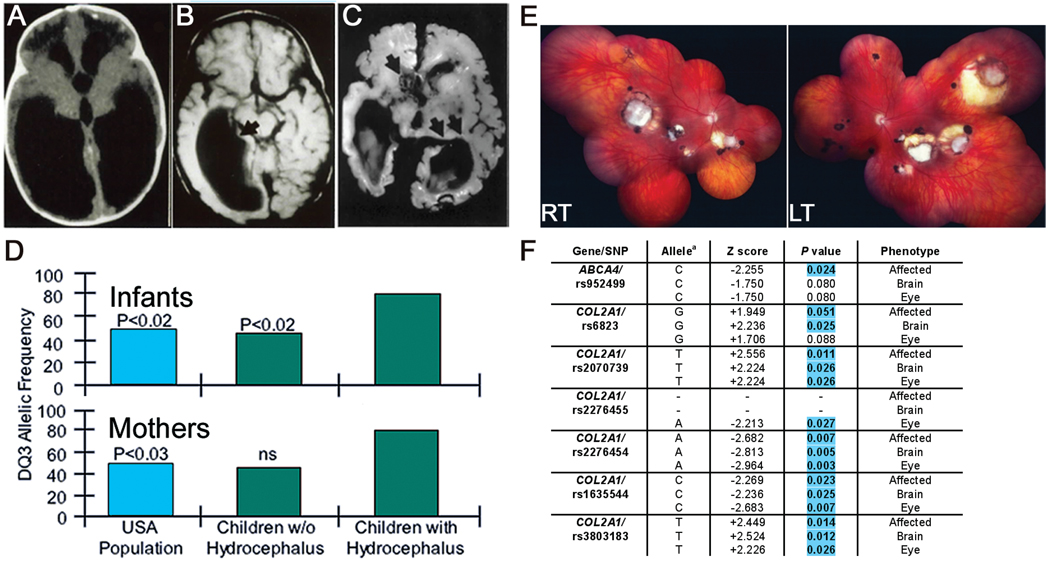
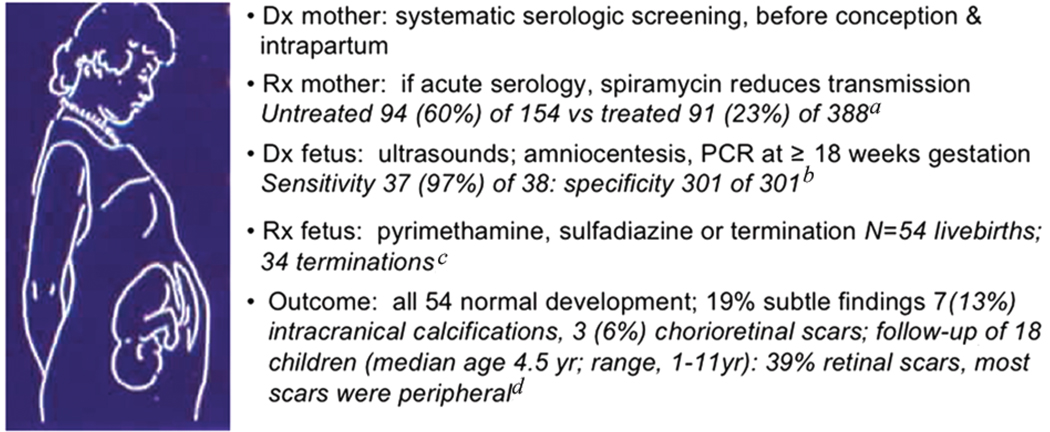
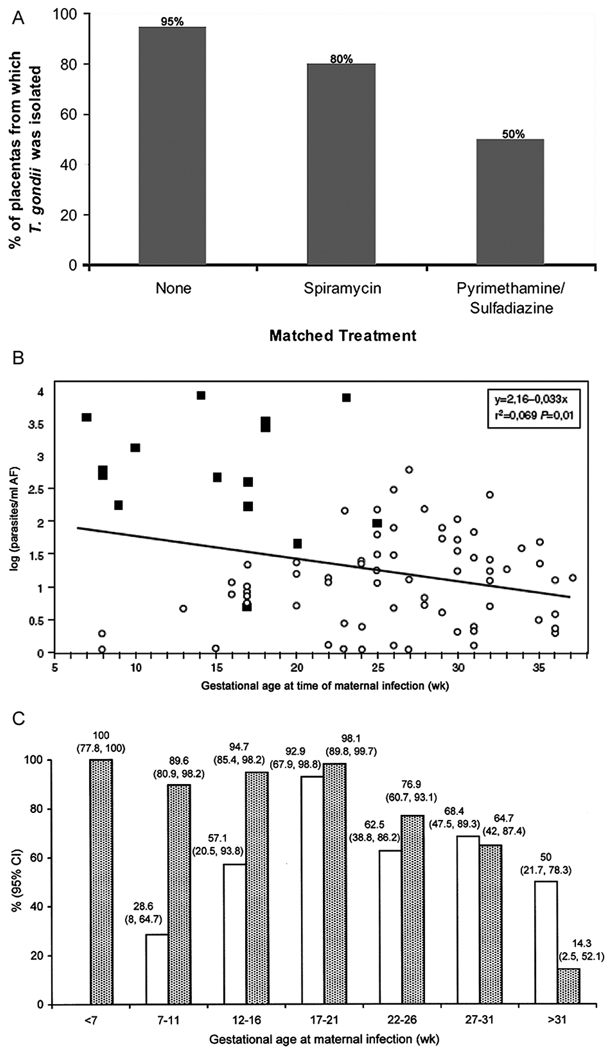
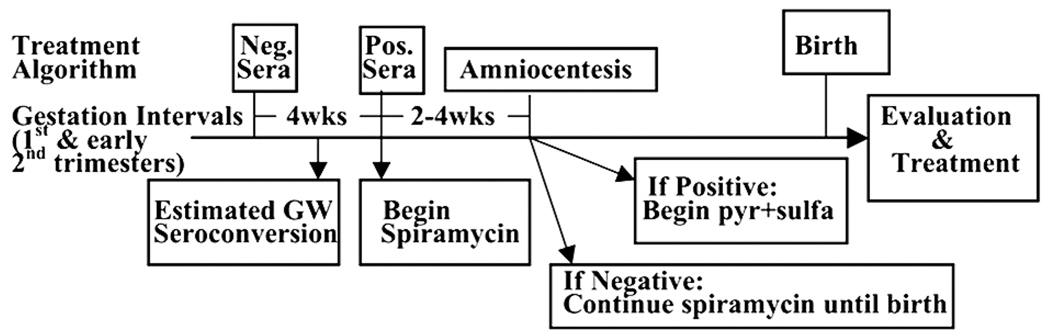
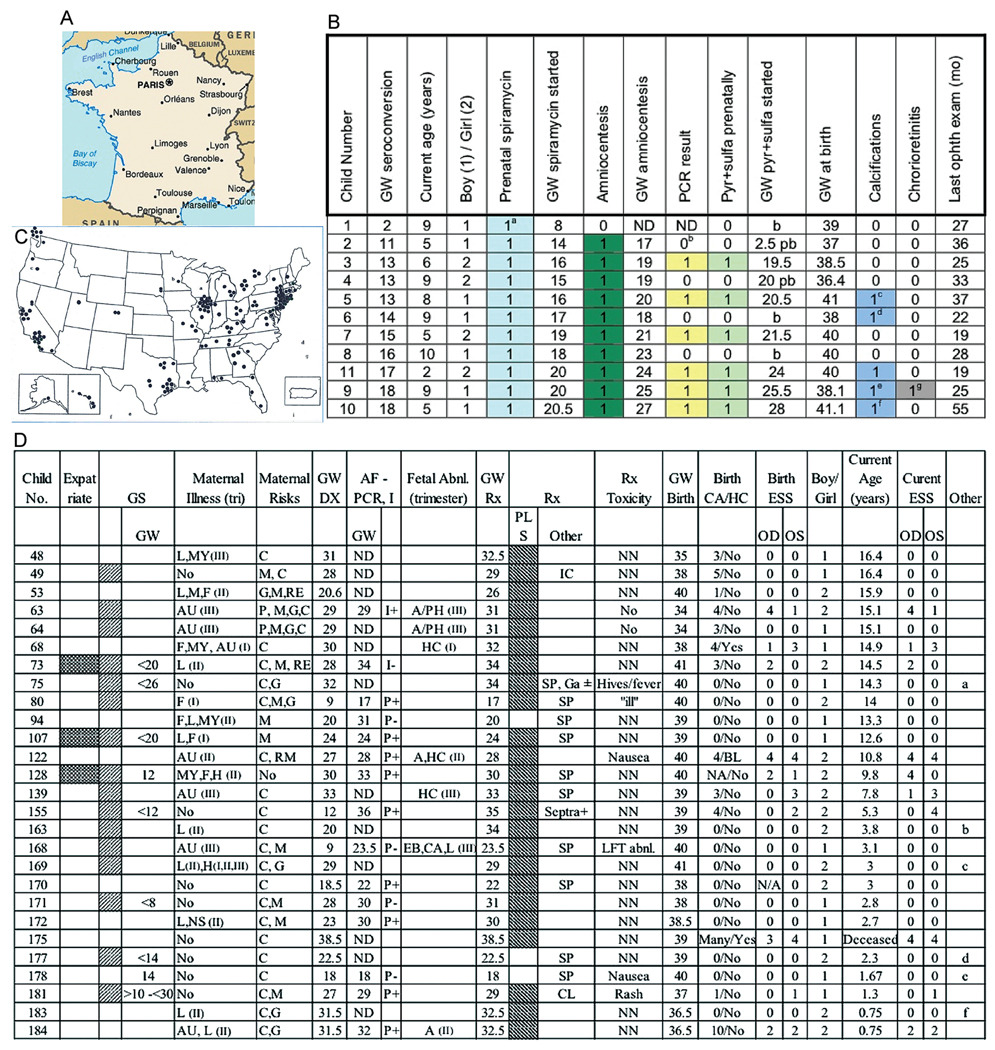
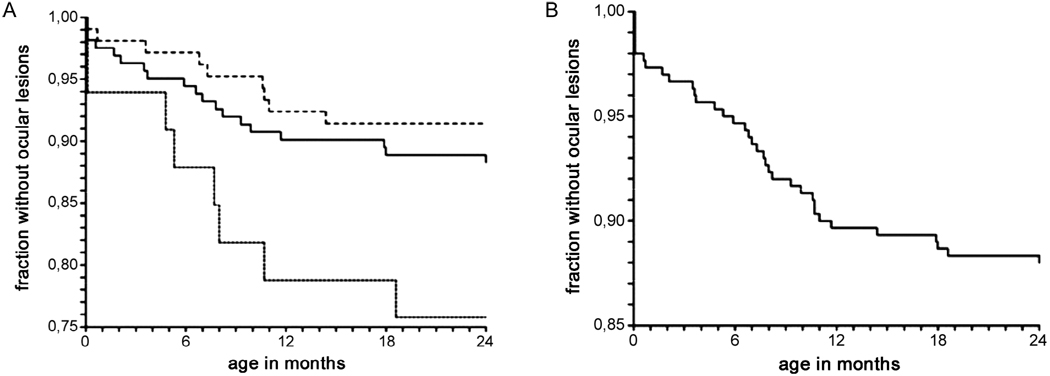
Evidence that prevention, diagnosis and treatment of toxoplasmosis is beneficial developed as follows: anti-parasitic agents abrogate Toxoplasma gondii tachyzoite growth, preventing destruction of infected, cultured, mammalian cells and cure active infections in experimental animals, including primates. They treat active infections in persons who are immune-compromised, limit destruction of retina by replicating parasites and thereby treat ocular toxoplasmosis and treat active infection in the fetus and infant. Outcomes of untreated congenital toxoplasmosis include adverse ocular and neurologic sequelae described in different countries and decades. Better outcomes are associated with treatment of infected infants throughout their first year of life. Shorter intervals between diagnosis and treatment in utero improve outcomes. A French approach for diagnosis and treatment of congenital toxoplasmosis in the fetus and infant can prevent toxoplasmosis and limit adverse sequelae. In addition, new data demonstrate that this French approach results in favorable outcomes with some early gestation infections. A standardized approach to diagnosis and treatment during gestation has not yet been applied generally in the USA. Nonetheless, a small, similar experience confirms that this French approach is feasible, safe, and results in favorable outcomes in the National Collaborative Chicago-based Congenital Toxoplasmosis Study cohort. Prompt diagnosis, prevention and treatment reduce adverse sequelae of congenital toxoplasmosis.
Figures
References
-
- Aagaard K, Melchior J. The simultaneous occurrence of congenital toxoplasmosis and congenital myxoedema. Acta Paedeatrica. 1959;48:164–168. - PubMed
-
- Ajzenberg D, Cogne N, Paris L, Bessieres MH, Thulliez P, Filisetti D, Pelloux H, Marty P, Darde ML. Genotype of 86 Toxoplasma gondii isolates associated with human congenital toxoplasmosis and correlation with clinical findings. J Infect Dis. 2002;186:684–689. - PubMed
-
- Alford C, Foft J, Blankenship W, Cassady G, Benton J. Sub-clinical central nervous system disease of neonates: a prospective study of infants born with increased levels of IgM. J Pediatr. 1969;75:1167–1178. - PubMed
-
- Alford CA, Schaefer J, Blankenship WJ, Straumfjord JV, Cassady G. A correlative immunologic, microbiologic and clinical approach to the diagnosis of acute and chronic infections in newborn infants. N Engl J Med. 1967;277:437–449. - PubMed
-
- Alford CA, Jr, Reynolds DW, Stagno S. Current concepts of chronic perinatal infections. In: Gluck L, editor. Modern Perinatal Medicine. Chicago: Year Book Medical Publishers; 1975. pp. 285–306.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
