

Isoniazid, rifampin, ethambutol, and pyrazinamide pharmacokinetics and treatment outcomes among a predominantly HIV-infected cohort of adults with tuberculosis from Botswana
- PMID: 19432554
- PMCID: PMC3762461
- DOI: 10.1086/599040
Isoniazid, rifampin, ethambutol, and pyrazinamide pharmacokinetics and treatment outcomes among a predominantly HIV-infected cohort of adults with tuberculosis from Botswana
Abstract
Background: We explored the association between antituberculosis drug pharmacokinetics and treatment outcomes among patients with pulmonary tuberculosis in Botswana.
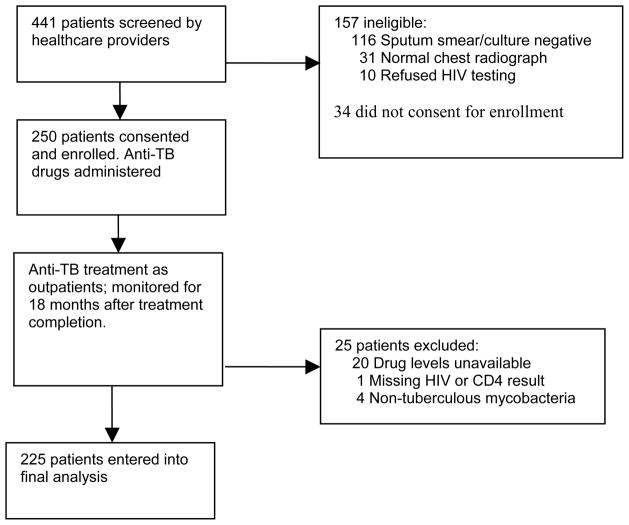
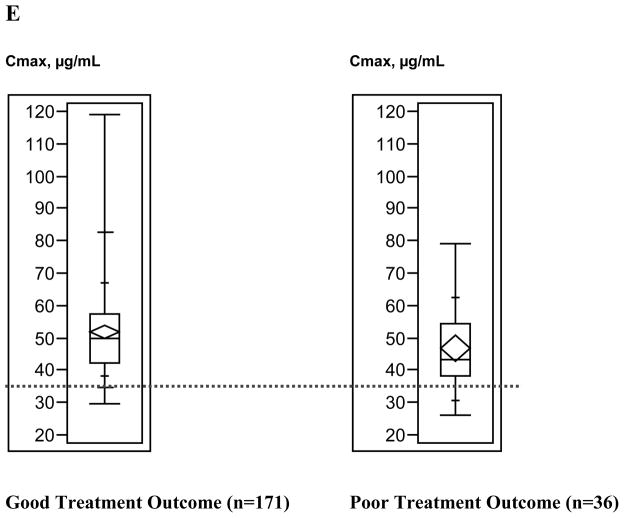
Methods: Consenting outpatients with tuberculosis had blood samples collected 1, 2, and 6 h after simultaneous isoniazid, rifampin, ethambutol, and pyrazinamide ingestion. Maximum serum concentrations (C(max)) and areas under the serum concentration time curve were determined. Clinical status was monitored throughout treatment.
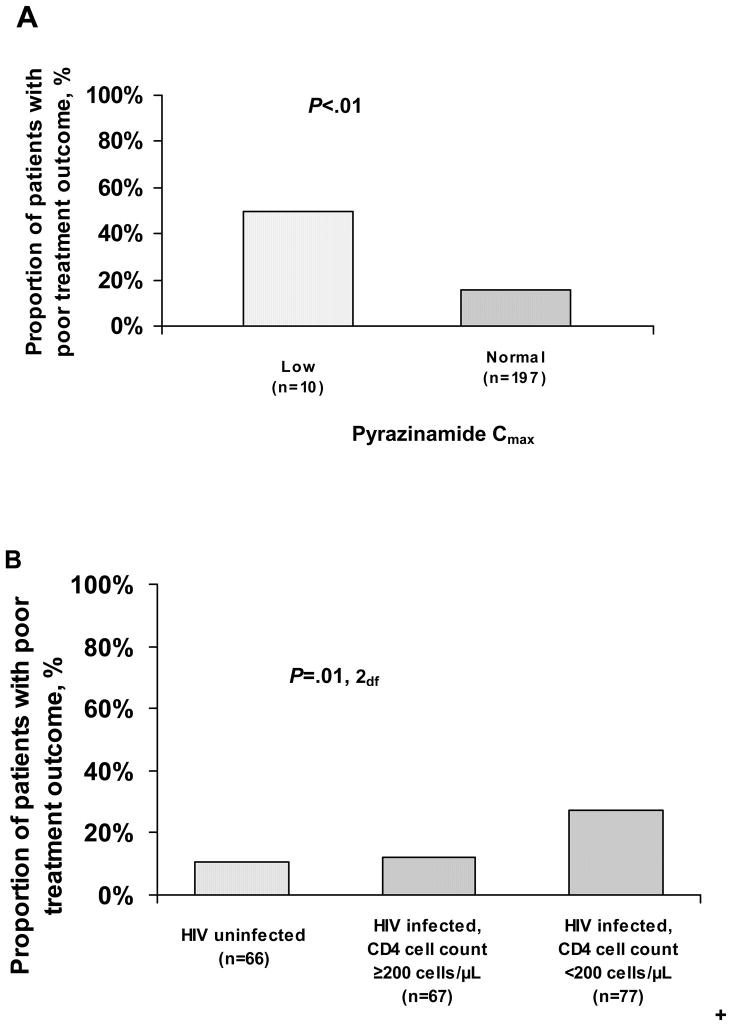
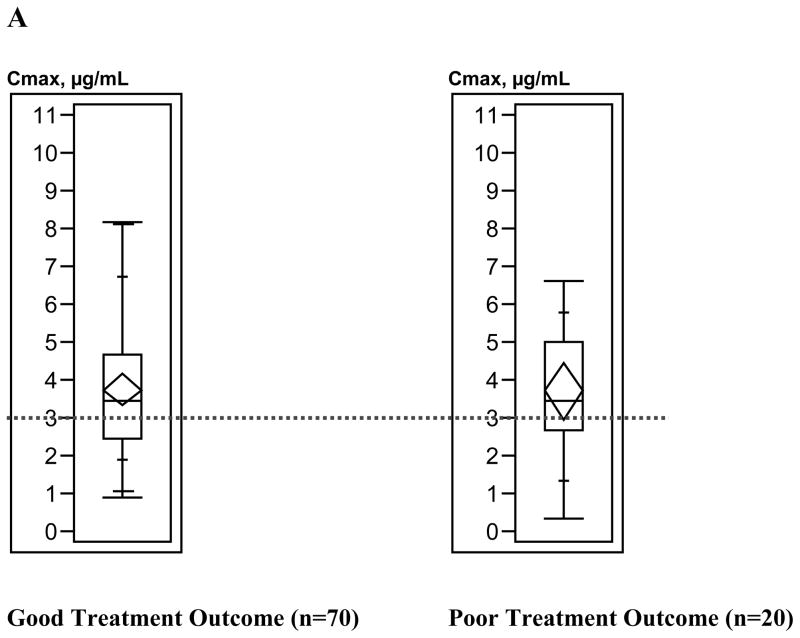
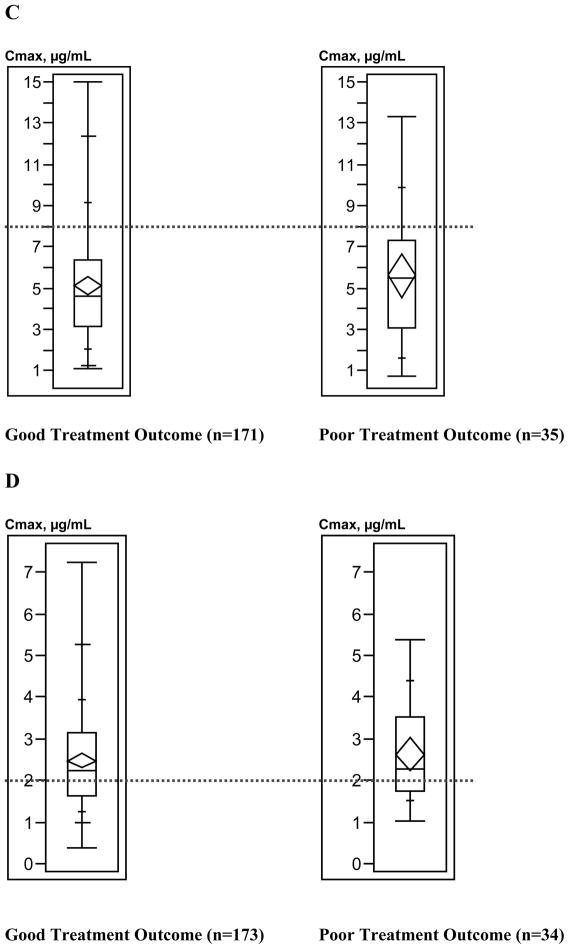
Results: Of the 225 participants, 36 (16%) experienced poor treatment outcome (treatment failure or death); 155 (69%) were infected with human immunodeficiency virus (HIV). Compared with published standards, low isoniazid C(max) occurred in 84 patients (37%), low rifampin C(max) in 188 (84%), low ethambutol C(max) in 87 (39%), and low pyrazinamide C(max) in 11 (5%). Median rifampin and pyrazinamide levels differed significantly by HIV status and CD4 cell count category. Only pyrazinamide pharmacokinetics were significantly associated with treatment outcome; low pyrazinamide C(max) was associated with a higher risk of documented poor treatment outcome, compared with normal C(max) (50% vs. 16%; P < .01). HIV-infected patients with a CD4 cell count <200 cells/microL had a higher risk of poor treatment outcome (27%) than did HIV-uninfected patients (11%) or HIV-infected patients with a CD4 cell count 200 cells/microL (12%; P = .01). After adjustment for HIV infection and CD4 cell count, patients with low pyrazinamide C(max) were 3 times more likely than patients with normal pyrazinamide C(max) to have poor outcomes (adjusted risk ratio, 3.38; 95% confidence interval, 1.84-6.22).
Conclusions: Lower than expected antituberculosis drug C(max) occurred frequently, and low pyrazinamide C(max) was associated with poor treatment outcome. Exploring the global prevalence and significance of these findings may suggest modifications in treatment regimens that could improve tuberculosis cure rates.
Conflict of interest statement
Figures

References
-
- Corbett EL, Watt CJ, Walker N, Maher D, Williams BG, Raviglione MC, Dye C. The growing burden of tuberculosis: global trends and interactions with the HIV epidemic. Arch Inter Med. 2003;163:1009–1021. - PubMed
-
- World Health Organization. [Accessed June 15, 2007];TB/HIV. http://www.who.int/tb/hiv/faq/en/index.html.
-
- Fox W, Ellard GA, Mitchison DA. Studies on the treatment of tuberculosis undertaken by the British Medical Research Council tuberculosis units, 1946–1986, with relevant subsequent publications. Int J Tuber Lung Dis. 1999;3(10):S231–S279. - PubMed
-
- Iseman MD. Tuberculosis therapy: past, present and future. Eur Resp J. 2002;20(Suppl 36):87s–94s. - PubMed
-
- Holdiness M. Clinical pharmacokinetics of the antituberculosis drugs. Clinical Pharmacokinetics. 1984;9:511–544. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
