

Increasing socioeconomic inequalities in first acute myocardial infarction in Scotland, 1990-92 and 2000-02
- PMID: 19432980
- PMCID: PMC2689199
- DOI: 10.1186/1471-2458-9-134
Increasing socioeconomic inequalities in first acute myocardial infarction in Scotland, 1990-92 and 2000-02
Abstract
Background: Despite substantial declines, Ischaemic Heart Disease (IHD) remains the largest cause of death in Scotland and mortality rates are among the worst in Europe. There is evidence of strong, persisting regional and socioeconomic inequalities in IHD mortality, with the majority of such deaths being due to Acute Myocardial Infarction (AMI). We examine the changes in socioeconomic and geographic inequalities in first AMI events in Scotland and their interactions with age and gender.
Methods: We used linked hospital discharge and death records covering the Scottish Population (5.1 million). Risk ratios (RR) of AMI incidence by area deprivation and age for men and women were estimated using multilevel Poisson modelling. Directly standardised rates were presented within these stratifications.
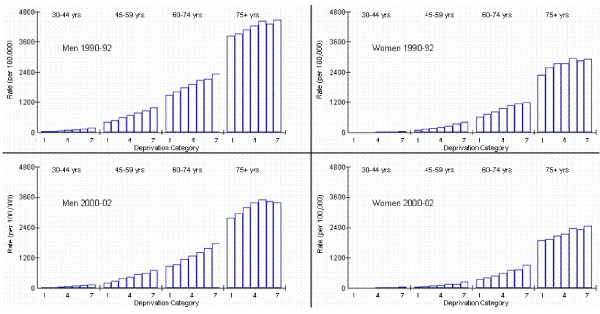
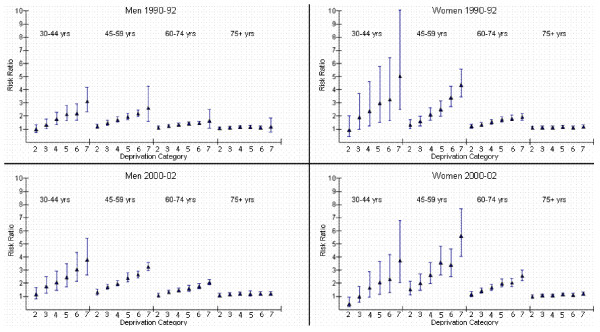
Results: During 1990-92 74,213 people had a first AMI event and 56,995 in 2000-02. Adjusting for area deprivation accounted for 59% of the geographic variability in AMI incidence rates in 1990-92 and 33% in 2000-02. Geographic inequalities in male incidence reduced; RR for smaller areas (comparing area on 97.5th centile to 2.5th) reduced from 1.42 to 1.19. This was not true for women; RR increased from 1.45 to 1.59. The socioeconomic gradient in AMI incidence increased over time (p-value < 0.001) but this varied by age and gender. The gradient across deprivation categories for male incidence in 1990-92 was most pronounced at younger ages; RR of AMI in the most deprived areas compared to the least was 2.6 (95% CI: 1.6-4.3) for those aged 45-59 years and 1.6 (1.1-2.5) at 60-74 years. This association was also evident in women with even stronger socioeconomic gradients; RRs for these age groups were 4.4 (3.4-5.5), and 1.9 (1.7-2.2). Inequalities increased by 2000-02 for both sexes; RR for men aged 45-59 years was 3.3 (3.0-3.6) and for women was 5.6 (4.1-7.7)
Conclusion: Relative socioeconomic inequalities in AMI incidence have increased and gradients are steepest in young women. The geographical patterning of AMI incidence cannot be fully explained by socioeconomic deprivation. The reduction of inequalities in AMI incidence is key to reducing overall inequalities in mortality and must be a priority if Scotland is to achieve its health potential.
Figures
Similar articles
-
Neighbourhood socioeconomic inequalities in incidence of acute myocardial infarction: a cohort study quantifying age- and gender-specific differences in relative and absolute terms.BMC Public Health. 2012 Aug 7;12:617. doi: 10.1186/1471-2458-12-617. BMC Public Health. 2012. PMID: 22870916 Free PMC article.
-
Income inequalities in case death of ischaemic heart disease in the Netherlands: a national record-linked study.J Epidemiol Community Health. 2012 Dec;66(12):1159-66. doi: 10.1136/jech-2011-200924. Epub 2012 Jun 8. J Epidemiol Community Health. 2012. PMID: 22685304
-
Trends and inequalities in short-term acute myocardial infarction case fatality in Scotland, 1988-2004.Popul Health Metr. 2010 Dec 6;8:33. doi: 10.1186/1478-7954-8-33. Popul Health Metr. 2010. PMID: 21134255 Free PMC article.
-
Psychosocial Factors and Recovery After Acute Myocardial Infarction in Younger Women.Curr Cardiol Rep. 2019 Apr 24;21(6):50. doi: 10.1007/s11886-019-1140-x. Curr Cardiol Rep. 2019. PMID: 31020453 Review.
-
Inequalities in care in patients with acute myocardial infarction.World J Cardiol. 2015 Dec 26;7(12):895-901. doi: 10.4330/wjc.v7.i12.895. World J Cardiol. 2015. PMID: 26730295 Free PMC article. Review.
Cited by
-
Neighbourhood socioeconomic inequalities in incidence of acute myocardial infarction: a cohort study quantifying age- and gender-specific differences in relative and absolute terms.BMC Public Health. 2012 Aug 7;12:617. doi: 10.1186/1471-2458-12-617. BMC Public Health. 2012. PMID: 22870916 Free PMC article.
-
Educational inequalities in acute myocardial infarction incidence in Norway: a nationwide cohort study.PLoS One. 2014 Sep 4;9(9):e106898. doi: 10.1371/journal.pone.0106898. eCollection 2014. PLoS One. 2014. PMID: 25188248 Free PMC article.
-
Socio-economic inequalities in rates of amenable mortality in Scotland: Analyses of the fundamental causes using the Scottish Longitudinal Study, 1991-2010.Popul Space Place. 2020 Sep 22;28(3):psp.2385. doi: 10.1002/psp.2385. eCollection 2022 Apr. Popul Space Place. 2020. PMID: 35411206 Free PMC article.
-
Stressors and resources mediate the association of socioeconomic position with health behaviours.BMC Public Health. 2011 Oct 13;11:798. doi: 10.1186/1471-2458-11-798. BMC Public Health. 2011. PMID: 21991933 Free PMC article.
-
Socioeconomic Status and in-hospital Mortality of Acute Coronary Syndrome: Can Education and Occupation Serve as Preventive Measures?Int J Prev Med. 2015 May 4;6:36. doi: 10.4103/2008-7802.156266. eCollection 2015. Int J Prev Med. 2015. PMID: 25984286 Free PMC article.
References
-
- Mackay J, Mensah G. The Atlas of Heart Disease and Stroke. World Health Organization; 2004.
-
- Information and Services Division Scotland 2005. http://www.isdscotland.org/
-
- Hanlon P, Walsh D, Buchanan D, Redpath A, Bain M, Brewster D, Cahalmers J, Muir R, Samlls M, Willis J, et al. Chasing the Scottish Effect: Why Scotland needs a step-change in health if it is to catch up with the rest of Europe. Public Health Institute of Scotland. 2001.
-
- Tunstall-Pedoe H, Kuulasmaa K, Mahonen M, Tolonen H, Ruokokoski E, Amouyel P. Contribution of trends in survival and coronary-event rates to changes in coronary heart disease mortality: 10-year results from 37 WHO MONICA Project populations. Lancet. 1999;353:1547–1557. doi: 10.1016/S0140-6736(99)04021-0. - DOI - PubMed
-
- Labarthe DR. Epidemiology and prevention of Cardiovascular Diseases: A Global Challenge. Aspen Publishers, Maryland, US; 1998.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
